Welcome to my site
Abstract
Suicide rates among veterans of the United States military remain a high-priority issue for the Department of Veterans Affairs (VA). Since 2007, there has been over 6,000 suicide deaths in the veteran community annually, an average of approximately 16 to 17 per day [1]. In response to this crisis, VA has implemented new policies and programs aimed at preventing suicides among veterans. However, these initiatives have failed to make any meaningful impact suicide rate despite increases to funding for mental health by Congress. This paper will examine the occurrence of suicide and the factors that put veterans at heightened risk over the nonveteran community. The impact of Congressional legislation on VA policy and funding will also be considered. This paper will also discuss VA’s response to the crisis, where it has fallen short, and finally, what improvements can be made to reduce the rate of suicide among veterans.
Common Acronyms
AFSP- American Foundation for Suicide Prevention
AI/AN- American Indian/Alaska Native
AMVETS- American Veterans
DAV- Disabled American Veterans
DoD- Department of Defense
ERPO- Extreme Risk Protection Order
GAO- Government Accountability Office
IAVA- Iraq and Afghanistan Veterans of America
IPTS- Interpersonal Theory of Suicide
NIH- National Institute of Health
OEF- Operation Enduring Freedom
OIF- Operation Iraqi Freedom
OIG- Office of the Inspector General
PTSD- Post-Traumatic Stress Disorder
TBI- Traumatic Brain Injury
VA- Department of Veterans Affairs
VCL- Veteran’s Crisis Line
VHA- Veterans Health Administration
VSO- Veteran’s Service Organizations
Introduction
Suicide is a phenomenon that has become all too familiar to members of the veteran community in the United States. When adjusted for age and sex, veterans die by suicide at 1.5 times the rate of non-veteran adults within the U.S.. Military personnel and veterans display several noticeable factors that put them at increased risk of suicide over civilians. Despite suicide prevention measures that have been implemented through federal programs, the rate of suicide death among veterans has shown no visible signs of decreasing.
The Department of Veterans Affairs (VA) is the agency responsible for the health care and wellbeing of veterans in the U.S. Over the past decade VA has instituted suicide prevention programs such as the Veteran’s Crisis Line (VCL) for veterans who are currently contemplating suicide and want to speak with licensed specialists. However, VA has faced strong criticism by lawmakers and veteran’s service organizations (VSO) who claim the organization is not taking a proactive approach in reducing the rate of suicide.
This paper will discuss the occurrence of suicide among U.S. veterans, such as what factors put them at increased risk and what methods have been proven to reduce the incidence of suicide. It will also discuss what measures VA, Department of Defense (DoD), and Congress have taken to reduce the rate of suicide as well as whether they have been effective or not. Finally, this paper will make recommendations on how VA can take a more proactive approach to reducing the rate of suicide among veterans.
The Phenomenon of Suicide
Suicide is defined the act or an instance of taking one’s own life voluntarily and intentionally. In 2018, 48,344 Americans died by suicide, making it the tenth-leading cause of death overall in the U.S.. Suicide is a growing problem within the U.S.; from 1999 to 2007 the rate of suicide death among the general U.S. population has increased 33 percent, from 10.5 to 14 per 100,000 people respectively. It is important to note that there is no single cause of suicide. Rather, suicidal ideation (the desire to die by suicide) stems from health, genetic, historical, and environmental stressors that can affect anyone at any period in their lives. Mental health stressors such as depression, substance abuse disorder, post-traumatic stress disorder (PTSD), and traumatic brain injury (TBI) are factors most commonly attributed to successful suicides. Despite its prominence as a national health concern, the act of suicide is still not a well understood phenomenon and preventative measures to reduce suicide rates are still an imperfect science with much room for improvement.
Warning Signs of Suicide
*Incomplete*
Health Factors of Suicide
Depression
Depression is a common but serious mood disorder that causes severe symptoms that affect how one feels, thinks, and handles daily activities such as sleeping, eating, and working. Depression can manifest itself in a number of ways including (but not limited to): persistent sadness/anxiety, feelings of hopelessness or pessimism, irritability, feelings of worthlessness or helplessness, loss of interest in hobbies, difficulty concentrating, and decreased energy or fatigue. Although the majority of people who have depression do not die by suicide, having major depression does increase suicide risk compared to people without depression. The Department of Health and Human Services has estimated that approximately 60 percent of people in the U.S. who die by suicide have a mood disorder such as major depression or bipolar disorder.
Substance Use Disorder/ Alcohol Use Disorder
Substance use disorders (SUD), particularly alcohol use disorder (AUD), influence suicidal behaviors and are linked to a substantial number of suicides and suicide attempts. The Substance Abuse and Mental Health Services Administration (SAMHSA) found in 2014 that approximately 1 in 12 individuals in the U.S. suffered from a substance abuse disorder in the past year and almost a quarter engaged in binge drinking within the last month. A study conducted by the Centers for Disease Control and Prevention (CDC) in 2010 found 22 percent of deaths by suicide involved alcohol intoxication at or above the legal limit. Similarly, acute alcohol intoxication was also present in about 30-40 percent of suicide attempts. Additionally, opiates were present in 20 percent of suicide deaths, marijuana in 10.2 percent, cocaine in 4.6 percent, and amphetamines in 3.4 percent. One reason alcohol and/or drug misuse significantly affects suicide rates in the disinhibition that occurs when a person is intoxicated. Alcohol abuse is also known to increase depressed moods and its availability makes it a prominent concern among suicide prevention researchers.
Post-Traumatic Stress Disorder
Post-traumatic stress disorder (PTSD) is a disorder that develops in some people who have experienced a shocking, scary, or dangerous event. It is natural to feel afraid during and after a traumatic situation, yet people who develop PTSD may continue to feel stressed or frightened, even when they are not in danger. PTSD is a disorder frequently associated with war veterans, however, anyone at any age can develop PTSD; symptoms of PTSD may manifest within three months of the traumatic incident but may sometimes begin years later. Trauma exposure and PTSD are well-established risk factors for suicidal thoughts and behaviors, with research indicating that comorbid [simultaneously present diseases or medical conditions] depression amplifies this risk. Because PTSD is one of the few psychological conditions that predict suicidal behavior among those who think about suicide, many patients with PTSD present clinically with elevate suicide risk.
Traumatic Brain Injury
Traumatic brain injury (TBI) is a sudden injury, such as a blow, bump, or jolt to the head that causes damage to the brain. The main causes of TBI are falls, vehicles crashes, sports injuries, child abuse, or blast injuries due to explosions. Penetrating TBI occurs when an object, such as a bullet or bone fragments from a skull fracture, enters the brain. Symptoms of TBI can be mild, such as a concussion; moderate; or severe. Most people completely recover from TBI, but severe cases can lead to serious psychical and psychological symptoms. Individuals with a history of TBI have been shown to have higher rates of nonfatal deliberate self-harm, suicide, and all-cause mortality than members of the general population. A study conducted over the course of 35 years in Denmark found those with medical contact for TBI compared to the general population without TBI had an increased risk of suicide with an incident rate ratio of 1.9:1[nearly twice as likely to die by suicide]. Additional analyses revealed that the risk of suicide was higher for individuals with severe TBI, numerous medical contacts, and longer hospital stays. The same study found that individuals were at the highest risk of suicide in the first six months after discharge.
Environmental Factors
*Incomplete* Economy and income, unemployment, relationship status, access to firearms
Historical Factors
*Incomplete* Prior suicide attempts, history of family violence/suicide, childhood abuse, neglect, trauma
Why are Veterans at Higher Risk of Suicide?
Suicide is an issue that, in general, affects veterans to a greater degree than non-veterans. The 2019 National Veteran Suicide Prevention (NVSP) Annual Report found that of the 45,390 American adults that committed suicide in 2017, 6,139 were veterans. By these metrics, 13.5% of the total suicide deaths were by veterans, despite the fact that veterans only make up 7.6% of the total population. Since 2007, the age-and-sex-adjusted suicide rate among veterans has increased from 18.5 per 100,000 to 27.7 per 100,000 in 2017. This increase in suicide deaths have occurred despite the fact that during this ten year period the total veteran population decreased by 18.3%. In comparison, the age-and-sex-adjusted suicide rate for the overall U.S. population in 2017 was 18.0 per 100,000 and the population grew by 17% during the same 10 year period.
There is no all-encompassing reason why a veteran would choose to die by suicide; rather, suicidal ideation and risk come from a variety of factors. Veterans who have recently separated from the military may be at risk of suicide due to the loss of camaraderie, the feeling of having no purpose, and a lack of fear or indifference towards death. Longer and more frequent deployments during the armed conflicts in Iraq and Afghanistan have taken a toll on younger veterans, as well as the stress related to combat devices such as improvised explosive devices and suicide bombers. Combat veterans are more likely to suffer from psychiatric disorders such as PTSD, depression, traumatic brain injury (TBI), bipolar disorder, substance abuse, and schizophrenia than those who did not experience combat and non-veterans. Approximately 25% of the total veteran population seen at VA hospital in 2010 reported suffering from at least one of these mental disorders. Additionally, 58.7% of veterans with recent VHA use who died by suicide in 2017 had a diagnosed mental health or substance use disorder.
The most common demographics at risk of suicide in the U.S. overall population are the same demographics that most commonly join the military: white, male, 18-34, and single. The 18-34 age bracket also has the highest rate of suicide in the veteran community at a rate of 45 per 100,000. It is important to note that while white men still comprise the majority of the military and veteran community, demographics are shifting as more minorities and women enlist. For most age groups, men have higher rates of use or dependence on illicit drugs and alcohol than women, though women are as likely as men to develop a substance abuse disorder.
Women Veterans
*Retool and rework entire section*
Access to Firearms
Access to firearms has been proven to increase the likelihood of suicide and nearly 70% of all veteran suicides are committed by firearms. Suicide attempts involving firearms are a particularly lethal means of self-harm, with a fatality rate of approximately 90%. However, gun ownership is incredibly popular in the military; nearly half of all veterans own one or more firearms. For this reason there has never been a concentrated effort to reduce the ownership of firearms by veterans who may be suffering from mental balance issues. Though clear links exist between firearm ownership and suicide risk, there has been a 20 year freeze on gun violence research in the U.S., which has resulted in a lack of empirical evidence. This 20 year freeze was recently ended in December, 2019, but only $25 million was dedicated as part of a $1.4 trillion deal signed by President Trump.
Military Stigma
Mental imbalance and suicidal ideation are significant risk factors of suicide that are not widely discussed within the military and veteran communities. The reluctance to share concerns about one’s own mental wellbeing is linked to a military culture that stigmatizes mental health care. Military culture prides itself on strength, and to admit mental distress is seen as a weakness that should be ignored. This is evidenced by the fact that 43% of veterans who died by suicide did not seek help from military treatment facilities or suicide hotlines in the month before their deaths. Suppression and avoidance of any instability, whether physical or mental, is a tactic taught in the military because, in the short term, they are powerful tools for adapting to the extreme adversity of combat. However, the concept that admitting pain makes one weak has consequences on veteran’s psyche long after they separate from the military, including not reaching out to mental health coordinators when experiencing mental instability.
Another aspect of military stigma that affects service members and veterans is the belief that pursuing mental health care could pose risks to one’s career or a fear of retribution. A common misconception among military communities is that seeking out mental health care of any kind could put their career at jeopardy or could cause their security clearance to be revoked. While it is true that certain psychological conditions could be grounds to revoke security clearance, a past or present mental, emotional, or personality disorder is not by itself a disqualifying condition to hold a security clearance. Likewise, speaking with mental health care professionals and participating in therapy are not disqualifying factors for a security clearance. The security concern arises when the possibility of future unreliable or dysfunctional behavior that could result in the willful or negligent compromise of classified information.
As attitudes towards mental health conditions have shifted towards acceptance in the mainstream consciousness, there has been a concerted effort by DoD and VA to dispel the stigma surrounding mental health care in the military. Military leaders have begun adopting tactics like discussing their own history with mental health conditions, promoting the belief that seeking help is a sign of strength, and educating service members on how to access mental health care. For this change in mindset to truly change the perception surrounding mental health, leaders from the top of the military to the bottom must be willing to change the way they acknowledge pain and suffering. There exists no empirical evidence that such a change in mindset would have an effect of the preparedness and training of the U.S. fighting forces.
Interpersonal Theory of Suicide
The Interpersonal Theory of Suicide (IPTS) proposes that the most dangerous form of suicidal desire is caused by the simultaneous presence of two interpersonal constructs- thwarted belongingness and perceived burdensomeness (and hopelessness about these states)- and further, that the capability to engage in suicidal behavior is separate from the desire to engage in suicidal behavior. Thwarted belongingness is comprised of a sense of isolation and a lack of meaningful and reciprocal relationships; perceived burdensomeness is comprised of self-hatred and a sense that others would benefit from one’s death more so than one’s continued life.
The concepts of thwarted belongingness and perceived burdensomeness are particularly relevant for veterans that have recently separated from the military. The life of a service member revolves around the concept of protecting the U.S. population and the freedoms it espouses; the importance of defending those interests is endlessly impressed upon every service member. Once the service member separates from that highly regimented lifestyle, the belongingness they felt of being a part of something bigger is stripped away and can weigh heavily on veterans. They quickly lose their existing support network of fellow service members and return to an area they have not lived in for a number of years. This sudden shift commonly results in veterans feeling alone and can spiral into isolation if left untreated, a common symptom of suicidal ideation.
The capability for suicide is comprised of an elevated tolerance for physical pain and a diminished fear of death and bodily harm. While genetics play a part in the capability for suicide, it is largely thought to emerge through repeated exposure to painful and/or provocative events, which lead to habituation to stimuli (e.g., pain, impending death) that would otherwise be highly aversive and serve as obstacles to suicidal behavior. The tolerance for any sort of pain is instilled on service members from the moment they begin initial training. In order to be successful in combat, one must learn to ignore pain and keep fighting until the enemy is defeated; this tenet is exemplified in the popular military ethos “train as you fight.” Service members must overcome pain quietly or risk being ridiculed as weak. While the American military approach of neglecting pain is effective in combat, it can have devastating consequences on veterans suffering from mental imbalance.
The Family Unit
The family unit can increase feelings of thwarted belongingness and perceived burdensomeness on veterans returning from deployment. Combat and non-combat deployments cause a great deal of stress on families of those deployed, and this stress likely contributes to family problems that arise during and after deployment. Stress within families does not end when the service member returns home from a deployment. Over 75% of married service members report some family readjustment issue post-deployment, with 66.6% reporting one or more concerns occurring on a weekly basis. Readjustment issues such as feeling like a guest in their own home, children being cold toward them, being unsure of responsibilities in the home, and intimacy issues are problems commonly reported in service members that return with any level of depression, PTSD, or generalized anxiety disorders.
Perceived burdensomeness is a significant risk for veterans with young children. Within the families of deployed service members, studies have found links between parental deployment and behavioral and academic problems in children, as well as child maltreatment and intimate spousal abuse. During long periods of absence, the deployed parent will inevitably miss milestones in their children’s development. It is not uncommon for children in these circumstances to not remember the deployed parent or may even be afraid of them. This can increase the anxiety on already struggling veterans and contribute to feelings of being a stranger within their own home. Feelings of being a stranger in the veteran’s own home can be compounded by the delegation of responsibilities with their spouse. After a 7-12 month deployment, service members return home and may be tempted to rush to return to the pre-deployment “normal.” During that absence the spouse has stepped up to handle all household and child-raising responsibilities. After doing things their way for so long, the spouse may be reluctant to relinquish control.
Suicide Rates Between Veterans and Non-veterans *Appendix A*
Veterans are not the only demographic who have seen an increase in suicide rates within the United States. Appendix A shows that between 1999 and 2018 the suicide rate increased by 35%, from 10.5 per 100,000 to 14.2 for a total of 48,344 deaths and an estimated 1.4 million suicide attempts in 2018. It is important to note during this timeframe the suicide rate increased by a rate of .8% per year from 1999 to 2006, and increased to 2.1% per year from 2006 to 2018. The increasing rate of suicide has made it the tenth-leading cause of death for all ages in the U.S., though it is the second-leading cause of death for those between 10-34 years old. To determine which groups are most at risk, the total suicide count can be broken down by four criteria: sex, age, race, and location.
Sex *Reference Appendix* *Appendix B*
The rate of suicide deaths by males comprises the majority of total suicide deaths; males are 3.5 times more likely than women to die by suicide on average. Between 1999 and 2018 the rate of suicide deaths by males rose 28%, from a rate of 17.8 in 1999 to 22.8 in 2018. During this same time period the rate of suicide deaths among women rose from 4.0 in 1999 to 6.2 in 2018 for an increase of 55%. As of 2017, males represent 79% of all U.S. suicides even though women attempt suicide three times as often as males. The reason for this imbalance can be linked to the method of suicide; firearms are the most common method used by males and are highly lethal, while females most commonly use less lethal means such as ingesting poison and suffocation.
There are direct correlations between the trends of suicide by sex between the nonveteran and veteran populations in the U.S. For instance, males die by suicide at much higher rates than women in both populations. Males are also more likely to use highly lethal means such as firearms, while women more frequently use less lethal means such as poisoning and suffocation. However, males and women veterans differ from their civilian counterparts regarding firearm suicide; both sexes in the veteran community are more likely to use firearms when dying by suicide. Additionally, women veterans die by suicide at a much higher rate (15.9 per 100,000) than nonveteran women, making it difficult to draw deeper inferences between the two populations.
Age *Appendix C*
Among the age brackets of 10-14, 15-24, and 25-34 suicide is the second-leading cause of death for an average of 16.74 per 100,000. However, broken down by age, the 55-64 age bracket has the highest incidence of suicide at 20.2 per 100,000 as of 2018, narrowly rising above the 45-54 age bracket where the rate of suicide is 20.04 per 100,000. According to the American Foundation for Suicide Prevention, younger groups have had consistently lower suicide rates than middle-aged and older adults. The incidence of suicide by age group in the nonveteran population does not show a correlation with the veteran population, where suicide rates are highest in the 18-34 age groups at a rate of 44.5 per 100,000.
Race *Appendix D*
In the U.S., White people die by suicide at rates much higher than any other race barring American Indians/Alaska Natives (AI/AN); White people also make up the majority of the U.S. population as well as the military and veteran community. In the medical community, there are several theories that may explain why White people die by suicide so frequently, but none are conclusive. The most frequently noted theory points to the ongoing opioid epidemic which largely affects white, rural communities.
Though they only make up 1.3% of the U.S. population, American Indian and Alaskan Natives have the highest rate of suicide among all ethnic groups in the country. According to the CDC these two indigenous populations die by suicide at a rate of 22.4 deaths per 100,000. Among the AI/AN veteran community the rate is even higher at 31.5 deaths per 100,000. In comparison, the rate of suicide among Black, Asian, and Hispanic nonveteran populations ranges from 6.9-7.1 per 100,000. The high incidence of suicide in AI/AN communities can be linked to existing health and societal disparities that negatively impact indigenous tribes in the U.S. Chief among these disparities is a lack of access to mental health care such as psychiatrists and psychologists. Alcohol abuse and untreated depression are high among AI/AN populations due to poor economic opportunities on reservations; autopsies performed on AI/AN suicides were much more likely to test positive for marijuana, alcohol, or amphetamines than White suicides.
There is a correlation between the rate of suicide by race in the nonveteran and veteran population of the U.S. White people and AI/AN people have far higher rates of suicide than Black, Hispanic, and Asian populations. Though there are culturally significant issues that must be noted, such as alcoholism among AI/AN people and opioid abuse among White people, geographic location may also play an important role. AI/AN communities are more likely to be rural if they are living within a reservation. Additionally, White people make up 77.8% of the total population living in rural communities in the U.S.. Geographic location and its impact on suicide rates will be explored in the next section.
Location *Appendix E*
The occurrence of suicide is much higher in rural Southern and Midwestern areas than in heavily developed and urban states in the Northeast and West. There are a number of contributing factors that explain this discrepancy. As previously stated, mental health services such as psychiatrists, psychologists and pharmacies can be scarce or non-existent in rural communities. Rural communities suffer from a shortage of mental health care professionals that are able to reside in each community which leads to long wait-times. Rural communities also tend to be spread out over large distances, creating many small and close-knit communities. Rural residents wishing to receive mental health care may sometimes have to travel hours to the nearest population center to receive care and may be forced to pay out of pocket for treatment when they do. Due to the close-knit nature of these small towns, lack of anonymity can also be a barrier to treatment out of fear of embarrassment or fear.
Rural communities also suffer from a similar mental health stigma that the military and veteran communities do. The fear of embarrassment or being labeled ‘crazy’ by one’s neighbors can be a powerful deterrent to seeking mental health care. The lack of anonymity in a small town may also cause fear of gossip amongst neighbors, though in general individuals in rural communities are similar to urban communities that they contribute neither positive or negative characteristics to a personal with depressive symptoms. Like the veteran community, individuals in rural areas may be less willing to admit the existence of depressive symptoms out of fear of the stigma they perceive is attached to mental health, despite evidence showing such a stigma is not attached to mental health care.
Conclusions on Nonveteran Suicide Statistics
There are many correlations between suicides in the nonveteran population and veteran population. White people have the second highest rate of suicide in the U.S. and have the highest rate of suicide in the veteran community. While AI/AN people have comparable rates of suicide, they make up a much smaller segment of the country, meaning the vast majority of suicide deaths in the U.S. are attributed to white people. Within the White population, there is large discrepancy regarding the rate of suicide between White males and White females; men of every ethnicity have much higher rates of suicide than women. The veteran community follows the same trend; White males make up the majority of suicide deaths. However, within the military and veteran community White males are disproportionately represented in comparison to the greater U.S. population by a wide margin. Up to a quarter of all White male veterans come from rural areas of the country that are often higher in poverty rates and lower in education rates than more developed areas of the country. When veterans return home to these rural areas, they may experience a lack of employment opportunities and appropriate health care relating to depression of suicidal ideation.
Suicide Prevention Methods
Psychotherapy, Outreach, Medication, Alternative therapies
USI Preventative Model (Not yet written)
Congressional Response to Elevated Veteran Suicide Rates
The responsibility for funding to VA and all mental health legislation falls on the two chambers of the U.S. Congress. Due to veteran’s status as a universally sympathetic group, veteran mental health is a perpetual high-priority target for legislation. Veterans are also a highly visible group; stories of veterans suffering with disability or dying by suicide elicit strong emotional reactions among the voting population that puts pressure on Congress to act. Both chambers of Congress have a Committee on Veterans Affairs where most legislation originates. However, legislators representing veteran-heavy districts may propose legislation based on dialogue with veterans in their constituency.
*New section on process taken to craft legislation focused on veteran suicide, including both chamber Committees/Subcommittees, lobbying by VSO’s, Congressional hearings? (could explain the emotional factor and contain it to one section)*
Joshua Omvig Veterans Suicide Prevention Act of 2007
Specialist Joshua Omvig was a soldier in the U.S. Army who died by suicide shortly after returning from an 11-month deployment to Iraq in 2004. A posthumous profile piece in Omvig’s hometown newspaper detailed the many symptoms of post-combat PTSD the soldier exhibited including nightmares, visible shaking, re-acclimatization issues, and the inability to discuss his experiences. In December of 2005, Omvig was arrested for drunk driving; he died by suicide in his vehicle the next day after being released from jail.
Omvig was far from the only high-profile suicide to occur during this time period. In 2007, Veterans for Common Sense filed suit on behalf of 320,000 to 800,000 veterans or their survivors against then-VA Secretary Jim Nicholson asking for relief in the form of immediate mental health treatment for veterans. In response, Congress drafted several bills ordering VA to take specific measures to improve mental health care for veterans, but none of the proposals made it through committee in either house of Congress. In early 2007, Rep. Leonard Boswell, the Democrat Representative of whom Omvig was a constituent, introduced the Joshua Omvig Veterans Suicide Prevention Act, which was seen as less specific and wide-ranging than previous legislative attempts, but would still require VA to address the problem of veteran suicide. The bill was signed into public law by President George W. Bush with 152 co-sponsors and unanimous votes in both the House and Senate.
The Joshua Omvig Veterans Suicide Prevention Act of 2007 (Omvig Act) is considered to be the first enacted piece of legislation specifically addressing veteran suicide. The Omvig Act (PL 110-110) ordered the Secretary of VA to develop and carry out a comprehensive program designed to reduce the incidence of suicide among veterans that included six specific provisions set forth by Congress. As part of the legislation, the VA Secretary was also required to submit a report within 90 days of the passage of legislation to provide a report to Congress containing information on the status of the implementation of the comprehensive program, the timeline and costs for complete implementation of the program, and a plan for additional programs and activities designed to reduce the occurrence of suicide among veterans.
The first requirement established mandatory training for appropriate staff, contractors, and medical personnel who interact with veterans that included information on recognizing risk factors of suicide, proper protocols for responding to veterans who may be at high risk of suicide, and best practices for suicide prevention. Though the Act did not prescribe a set of best practices, it required VA to conduct research in conjunction with the HHS, NIMH, SAMHSA, and CDC to determine the best practices in veteran suicide prevention.
The second requirement in the Omvig Act requires VA medical staff to offer mental health evaluations in their overall health assessment and to provide referrals (at the veteran’s request) to appropriate counseling and treatment programs for veterans exhibiting symptoms of mental health problems. This provision reduced the barriers frequently encountered by veterans seeking mental health care who did not have a documented mental illness but exhibited symptoms of suicidal ideation.
The Omvig Act also called for the designation of suicide prevention counselors at each VA medical facility. The legislation outlined the role of suicide prevention counselors as one who works with local emergency rooms, police departments, mental health organizations, and veterans service organizations to engage in outreach to veterans and improve the coordination of mental health care to veterans. The establishment of this position allows VA facilities across the country the ability to work with local resources to reach out and provide care to veterans who may not be enrolled in the VA health system but may be experiencing a mental health crisis, including homeless veterans.
The fourth requirement of the Omvig Act called for the VA Secretary to provide research on mental health care for veterans who have experienced sexual trauma while in military service. Military sexual trauma (MST) is a systemic problem within the military; while men do experience MST, the problem is less far-reaching than women veterans who experience MST at much higher rates.
One of the most successful initiatives to come out of the Omvig Act is the establishment of the Veterans Crisis Line (VCL). The VCL is a 24/7 free, anonymous, confidential resource that is available to all veterans, service members, family members, and friends regardless of enrollment in VA. Veterans who contact the VCL speak with qualified responders specially trained and experienced in helping veterans of all ages and circumstances. VCL responders listen to the veteran and, when applicable, provide resources for further care or initiate the dispatch of emergency services to callers in crisis. Since its establishment in 2007 the VCL has handled more than five million calls and has dispatched emergency services to callers in crisis more than 159,000 times. Additionally, VCL has provided more than 897,000 referrals to VA suicide prevention coordinators to make it easier for veterans to receive more permanent assistance. In 2009 the VCL was expanded to support online chats; to date VCL has handled more than 585,000 online chats. In 2011 the VCL was further expanded to support text-message services and has since handled more than 184,000 conversations with veterans who did not wish to speak directly.
The sixth and final requirement of the Omvig Act pertains to outreach and education for veterans and their families with a special emphasis on OIF and OEF veterans. The educational programs created through this provision were designed to remove the stigma associated with mental illness, encourage veterans to seek treatment and assistance for mental illness, and to promote skills for coping with mental illness. Additionally, educational programs were created aimed at helping the families of veterans in understanding the issues arising from the readjustment of veterans to civilian life, identifying the signs and symptoms of mental illness, and encouraging veterans to seek assistance for mental illness.
Though it was not included as a requirement under the comprehensive suicide prevention program, Congress also encouraged the VA Secretary through the Omvig Act to create a volunteer peer support counseling program. From this recommendation, VA created the Peer Support Mentoring Program to link veterans with veteran mentors who have experienced similar challenges and situation. Under the peer support program, veterans are trained to conduct outreach to veterans and their families as well as adequately assist other veterans with issues related to mental health and readjustment. Veteran mentors do not only serve as a friend and a good listener, but also as someone who can provide first-hand experience in navigating the intricacies of the VA health system. The success of the Peer Support Mentoring Program has prompted many prominent VSO’s to create their own version of the program for its members to connect together.
Clay Hunt Suicide Prevention for American Veterans Act
While the Joshua Omvig bill was the first step, the legislation that has led VA to where it is currently is the Clay Hunt Suicide Prevention for American Veterans Act (Clay Hunt SAV Act). The Clay Hunt SAV Act is named for Sgt. Clay Hunt, a Marine sniper who took his life in 2011, just two weeks after seeing a VA psychiatrist. While Joshua Omvig’s story dealt with the effects of undiagnosed PTSD, Clay Hunt’s story focused on VA’s failure to help him when he reached out. Congressional testimony provided by Hunt’s mother highlighted how, despite his pro-active approach to seeking health care, he struggled to get appointments with a psychiatrist and felt like a guinea pig as a variety of medications were tried to treat his PTSD. The Clay Hunt SAV Act represented the chance to make substantial change within VA, a move President Obama was eager for in the wake of the 2014 Phoenix Waiting Room scandal.
The first provision of the Clay Hunt SAV Act established a yearly third-party evaluation of VA’s mental health care and suicide prevention programs. The annual mental health care report uses metrics common among mental health care practitioners and identifies the most effective programs conducted through VA for suicide prevention. The yearly report also provides information on the cost-effectiveness of these programs and evaluates the level of patient satisfaction with respect to their involvement in any VA program. Finally, the report provides systematic updates to and recommendations for best practices regarding veteran mental health and suicide prevention.
The second provision of the Clay Hunt SAV Act required VA to survey the Department’s existing websites and information resources to create a centralized website that serves to provide veterans with information regarding all of the mental health care services provided by VA. In addition to serving as a singular point of information, the Act requires that the website contain information on resources available to veterans within their regional VA network, including the name and contact information of local social work offices, mental health clinics, and a list of appropriate medical staff. The website, mentalhealth.va.gov, has grown since its inception and now provides veterans and their families with a local resource finder, informative pages covering all forms of mental illness, and support resources for specific types of veterans and civilians. The final requirement of this provision ensures all information and sources available through VA’s centralized website are updated and corrected no less than every 90 days or as more current information becomes available.
The third provision called on the VA Secretary to establish a pilot program that repaid the educational loans for certain psychiatrists working for VHA within three years. Under this pilot program, individuals licensed or eligible for licensure to practice psychiatric medicine, as well as those enrolled in the final year of a residency program leading to specialty qualification in psychiatric medicine, would be eligible to have their student loans repaid. Individuals participating in this program would be required to enter into a period of obligated service of two or more years with VHA in the field of psychiatric medicine.
The fourth provision called on the VA Secretary to establish a pilot program to assist veterans transitioning from serving on active duty and to improve the access of veterans to mental health services. Under the pilot program a community oriented veteran peer support network would be established within certain VISN’s to help veterans navigate VA’s resource and benefits system. Additionally, a community outreach team would be created at medical centers with the aim of assisting veterans transitioning into communities, facilitate outreach activities between veterans and their communities, and act as liaisons between veteran and local resources such as legal aid.
The fifth provision of the Clay Hunt SAV Act eliminated bureaucratic red-tape between VA and non-profit mental health organizations to improve the efficiency and effectiveness of suicide prevention efforts. The elimination of bureaucratic barriers allows for trained VA medical professionals to lend their expertise to local suicide prevention non-profits through best practices and collaboration to exchange training sessions between organizations.
The final provision of the Act, included to appease Congress people opposed to government spending, prohibited any new appropriations for the reforms to be implemented within VA. Instead, VA was forced to cannibalize its own budget and pull funding away from other projects to complete requirements such as the centralized website. In the five years since the SAV Act became law, VA has submitted to Congress a yearly report of the pilot programs the Act established. Veteran’s service organizations such as American Veterans (AMVETS) and the Iraq and Afghanistan Veterans of America (IAVA) have provided significant pushback against VA over the findings of the report as well as recommendations on how to address systemic problems in the agency. An IAVA report published in 2019 found that the loan repayment pilot program and the transition assistance pilot program have suffered from a lag in funding because no additional funds were allocated to VA by Congress. The same report found that increases in funding for mental health care through the Trump Administration budget have recently allowed these programs to get underway.
Choice Act
During the same time period as the Clay Hunt SAV Act, feelings of frustration in the public over veteran health care were exacerbated by outrage over the 2014 “Waiting List” scandal. In April 2014, a CNN investigative report found that hospital directors at a Phoenix, Arizona VA hospital were keeping secret waiting lists of veterans seeking appointments with their primary care physician. These waiting lists were hidden from federal regulators to produce lower average wait metrics, which resulted in the potentially preventable deaths of at least 35 veterans. The public outcry over the scandal eventually led to the resignation of VA Secretary Eric Shinseki and amplified calls for reform within the organization.
From this scandal, the Veterans’ Access to Care through Choice, Accountability, and Transparency Act of 2014 (Choice Act) was signed into law by President Obama on 7 August, 2014. The Choice Act provided veterans with the option to get non-VA health care from community providers paid for by VA if they live more than 40 miles from a VA medical facility or if they must wait more than 30 days to receive an appointment at VA hospitals. While it was not mental health-specific in nature, the Choice Act gave veterans options outside VA where they could receive health care and mental health care. Additionally, the Choice Act dedicated $500 million in funding to hire more doctors and nurses at VA hospitals, which helped to reduce staffing shortages and lagging pay scales among employees. The Choice Act ran out of funding in May 2018 and was replaced by an expanded version of the program, named the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks Act of 2018 (MISSION Act), signed into law by President Trump in June 2018.
MISSION Act
Under the MISSION Act, the Choice program was expanded to consolidate community care programs, create better customer service, provide new urgent care benefits, and modernized IT systems within VA. The MISSION Act also altered the distance requirements to use the Choice program, changing it from a 30 mile distance to a 30 minute average drive for primary care, mental health, and non-institutional extended care services. The MISSION Act was implemented on June 6, 2019, though it is too early to conduct a thorough analysis.
Commander Scott Hannon Veterans Mental Health Care Improvement Act
The Commander Scott Hannon Veterans Mental Health Care Improvement Act (S. 785) was passed by both chambers of Congress on September 25, 2020. The bill will now travel to the desk of President Trump, who is expected to sign the legislation into law. The Hannon Act gained the support of the White House, VA, dozens of veteran’s service organizations, and Republican and Democratic lawmakers. The legislation, considered by Senator Jerry Moran to be the most significant bill regarding veteran’s mental health care to come out of the committee. The Hannon Act will provide funding for increased research into mental health problems, and will consider a number of nontraditional therapy methods, including hyperbaric oxygen therapy, animal therapy, agritherapy, and art therapy among others.
The Hannon Act will also provide critical funding to increase staffing in VA hospitals and will introduce a pilot program to provide grants for those working at vet centers across the country. An important piece of the legislation will also create independent oversight on VA’s outreach campaign, which has seen far less engagement in the past two years than at its peak in 2016. One other notable portion of the Hannon Act includes legislation specifically relating to women veterans. Under the legislation VA must create a centralized website for women veterans to access all benefits and resources that apply to them, including counseling for MST.
Veterans Affairs
The Department of Veterans Affairs is the federal executive branch that oversees all issues pertaining to veterans and their health care. VA is comprised of three separate administrations: the Veterans Health Administration, Veterans Benefits Administration, and the National Cemetery Administration. The Cabinet-level organization is headed by the Secretary of Veterans Affairs, a position chosen by the president and confirmed through vote in the Senate. The current Secretary of Veterans Affairs, Robert Wilkie, was nominated by President Trump and confirmed in the Senate in July 2018.
Of the three organizations comprising the VA, the Veterans Health Administration (VHA) oversees veteran health care, research and the training of physicians through affiliations with educational institutions. VHA serves over 9 million enrolled veterans annually at 1,255 health care facilities. The responsibility of addressing and reducing the incidence of veteran suicide falls on VHA. Where funding is concerned, VA and DoD combined are the third largest research authorities on suicide prevention, behind NIH and the American Foundation for Suicide Prevention (AFSP) (NAASP 12). Primary oversight for VHA is provided by VA’s executive branch, the Government Accountability Office (GAO), the Inspector General of Veterans Affairs, and the House and Senate Committees on Veterans Affairs.
New Regulations and Legislation Implementation
The rules and regulations of VA and VHA are constantly changing as new research is conducted and “best practices” standards evolve. In the VA Executive Office, the Office of Regulation Policy and Management is responsible for the formulation and control of all VA regulations. The Office of Regulation Policy and Management provides a centralized management and control structure that reports directly to the Secretary and Deputy Secretary of Veterans Affairs. Among areas under its purview, the Office conducts comprehensive overview, reorganization, and rewriting of VA’s existing regulations; it also works with the Office of Congressional and Legislative Affairs to implement new legislation and initiatives such as pilot programs.
The Office of Congressional and Legislative Affairs is the focal point for VA management and coordination of all matters involving Congress. The two offices work together under the direction of the VA Secretary to create pilot programs authorized through enacted Congressional legislation to explore new methods of treating veteran mental illnesses. Pilot programs conducted at individual VA hospitals that demonstrate positive results are referred back to the Office of Regulation Policy and Management to be implemented across all VA hospitals and outpatient facilities.
Criticism of Veterans Affairs
Due to its nature as a highly visible Cabinet-level department, VA has received significant scrutiny by veterans, VSOs, the news media, Congress, and government oversight organizations. Criticism of VA tends to revolve around certain topics: struggles with staffing, wait times, funding, information systems such as electronic medicals records, gender and minority health care disparities, and lack of uniform standards enforced at individual hospitals. While VA has committed itself in recent years to addressing these systemic failures, the process has experienced setbacks as well as successes.
One of the core issues affecting reform within VA is funding. Pilot programs for new methods of treating veterans and attracting staff have not received adequate funding, which has led to delays in implementation and results. The issue of funding may not be that it is inadequate, but rather that funds appropriated to VA have a too-narrow scope. Congress appropriates VA’s budget as a nondefense discretionary program, thus, Congressional priorities can influence both the level of money available and the way VA may spend the money once allocated. For example, programs in VA may be left underfunded despite the availability of excess funds in other initiatives because those funds have been specifically earmarked by Congress. This level of bureaucratic red-tape is typical of any large agency, but it has stymied the organization from making much needed reforms. Since 2016 there has been a concerted effort to cut red tape by eliminating outdated VA policies and streamlining the funding process.
Staffing at VA hospitals is another area where VHA receives continuing criticism. This issue affects every level of VA, from nurses in rural VA locations to Medical Directors managing entire VA hospitals. An OIG report released September 2019 found 96% of VHA facilities reported at least one severe occupational shortage, 39% of which noted at least 20 severe occupational staffing shortages. The same OIG report found that VA has difficulty hiring Medical Directors to hospital due to the high stress of the position, a salary lower than the private sector, unclear recruiting processes, and career risk due to negative publicity. Having high turnover rates and vacancies in the highest position in a VA hospital exacerbate issues like uneven standards of care and wait times that cause the organization to draw such negative attention.
Despite updates to pay scales for VA hospital workers, nearly 40,000 of the 335,000 positions in the Veterans Health Administration are still vacant. The majority of these vacancies reside in densely populated areas such as Los Angeles, California and deeply rural states like Montana and Colorado. Historically lower pay scales have made it difficult to attract medical professionals to less populated areas, which can increase wait times or make some services unavailable in particular areas. Fortunately, there has been improvement in this area under the MISSION Act, signed by President Trump, which increases pay scales to make VA positions more attractive. Pilot programs such as the student loan repayment program for psychiatric medicine graduates have the potential to fill these vacancies if they are implemented through the entire VA organization. This pilot program is currently ongoing and its feasibility has not yet been established.
The Trump Administration
Under the Trump Administration, VA has been marked by record turnovers and vacancies of leadership that have had negative effects on the agency. Over the past five years, VA has had four different Secretaries and four more acting Secretaries. Additionally, VA’s top health official post, Under Secretary for Veterans Health Administration, has been vacant since President Trump took office. The most recent example of turmoil in VA leadership under President Trump came when VA’s second ranking official, Deputy Secretary of Veterans Affairs James Byrne, was abruptly removed from office after just five months in the position. Byrne was dismissed by Secretary of Veterans Affairs Robert Wilkie, who declined to give any reason for the removal outside a ‘loss of confidence.’
These abrupt changes in leadership are having a direct effect on VA’s ability to provide mental health care to veterans at risk of suicide. The lack of consistency among leadership and the vacancies of top positions were highlighted in a 2018 GAO report that found senior leadership has lacked the stability needed to ensure issues policy meets agenda goals. The report shows funding for outreach content for social media had been increasing from 2013 until it peaked in 2016. After the 2016 peak, that outreach declined steeply, and was on track to be below 2013 levels by 2018. Research has shown that outreach programs are effective in preventing suicide; reducing outreach could increase feelings of loneliness among veterans. Outreach by VA is vital to the mission of suicide prevention; as many as 52% of veterans are not enrolled in VA or VHA. When a veteran sees an advertisement or public safety announcement regarding their mental health, they may remember they are not alone and reach out to VA or VCL for help.
On June 17, 2020, President Trump unveiled the President’s Roadmap to Empower Veterans and End a National Tragedy of Suicide (PREVENTS). PREVENTS is an interagency task force intended to reduce bureaucratic red-tape and consolidate federal suicide prevention efforts into one comprehensive nationwide strategy. While the PREVENTS task force does not include physical legislation, it does provide a series of recommendations that will be implemented across VA as well as other federal programs. Central to the task force are reforms to how suicide prevention research is conducted. PREVENTS will identify and prioritize suicide surveillance and research that focuses on a veteran’s unique combination of individual, relationship, community, and societal factors to deliver the most effective intervention(s) tailored to meet their needs and circumstances. Additionally, the program will promote foundational changes to the way research is conducted- including improving the speed and accuracy with which research is translated into practice, improving efficiency through data sharing and data curation practices, and using innovative funding techniques to drive team science and reproducibility.
PREVENTS is also intended to reduce bureaucratic red-tape by developing partnerships across government agencies and nongovernment entities and organizations to increase capacity and impact of programs and research to empower veterans and to prevent suicide. These initiatives will be funded through an interagency federal funding mechanism working with suicide prevention programs at both the federal and local level. The PREVENTS task force has practical improvements for suicide prevention programs and research that may benefit veterans by helping VA avoid future bureaucratic constraints that have historically hamstrung the process. Critics of the PREVENTS task force include Senators Jon Tester, Jerry Moran, and Rep. Mark Takano, who claim the initiative does not provide enough concrete steps to legislate policy changes. Rep. Takano stated that PREVENTS amounts to “Tepid calls for more research, interagency coordination and meek public education campaigns won’t do enough to end this crisis,”. While PREVENTS is a White House program, Congressional leaders on the House and Senate Committees on Veterans’ Affairs have promoted the recently Congressionally-passed Commander Scott Hannon Veterans Mental Health Care Improvement Act.
Funding for Suicide Prevention
Suicide is still not a well understood phenomenon and research into the subject has not been adequately funded. The lack of adequate funding for suicide prevention research extends beyond VA and includes civilian research. Despite being the 10 leading cause of death among Americans, research into suicide prevention receives a fraction of funding that other issues do. For example, the National Institute of Health (NIH) found that from the time period of 2008 to 2013, approximately $430 million was dedicated to suicide research. However, in 2016 alone $500 million was spent on alcoholism research and $690 million on breast cancer research. To put that into comparison, 45,000 Americans die by suicide each year and 65,000 die from alcoholism.
The NIH report, “U.S. National Suicide Prevention Research Efforts: 2008-2013 Portfolio Analysis” shows that of the 383 studies done on suicide prevention during this timeframe, the NIH conducted 156 studies, the AFSP conducted 99, and VA/DOD conducted 82 combined. The AFSP hopes to use these studies to establish a system of best practices aimed at drastically reducing the annual rate of suicide by 2025. The initiative, named Project 2025, will create a predictability model to determine which prevention methods could have the greatest impact, and establish benchmarks to measure against for the next 10 years. The four phase program will take those findings and develop specific strategies for reducing the rate of suicide, and collaborate with other suicide and mental health organizations to focus their prevention efforts on the kinds of programs, policies, and interventions that will save the most lives in the shortest amount of time. The associate director of the Center of Excellence for Suicide Prevention within VA sits on the 17-member advisory committee for Project 2025.
How Suicide Prevention Research is Conducted
Research for suicide prevention is conducted through multiple federal agencies every year. In the U.S., three federal agencies conduct the majority of suicide prevention research: NIH, DoD, and VA. Among these agencies, the NIH has the greatest capacity to conduct research into suicide prevention; the DoD is second-highest and is closely followed by VA. While it is not a federal agency, the AFSP funds more research into suicide prevention more than both the DoD and VA through private donations. Smaller public health organizations, such as the Substance Abuse and Mental Health Services Administration and the Brain & Behavioral Research Foundation, also conduct research into suicide prevention, though their studies are smaller in scope than larger federal agencies.
At the surface level, it may seem redundant to have multiple federal agencies all conducting independent research into suicide prevention. However, all federal agencies are funded independently of each other through Congress’ yearly budget and do not compete for resources. Rather, each agency conducts research relevant to the populations they oversee. For instance, studies funded through the NIH pertain to suicide and suicide prevention among the total U.S. populace, of which active-duty military and veterans represent a small percentage. Research studies funded and conducted through VA pertain only to veterans and their immediate family. Likewise, research conducted through the DoD uses active-duty and reserve military as their sample population.
The results of all peer-reviewed studies and research conducted through federal agencies such as the DoD and VA are all published on the PubMed website, run by the NIH, no later than 12 months after results are released. Publishing results of studies under one agency makes it easier for researchers to use previous information gathered from other entities to increase their sample size while cutting out redundant bureaucratic red-tape. The PREVENTS Roadmap unveiled under President Trump seeks use shared information between agencies to create a comprehensive nation-wide suicide prevention program that also includes research conducted by private entities. The goal of sharing results between agencies under the PREVENTS Roadmap will identify biomarkers in active-duty military, veterans, and civilians that will predict suicidal ideation and risk factors among all groups that may otherwise go unnoticed.
Conclusion and Recommendations
Based upon the evidence presented in this report, there are several areas that represent the biggest challenges facing VA in reducing the rate of suicide among veterans. The first area of concern involves the funding appropriated to mental health care research and the number of studies that are conducted. Suicide is still a relatively unknown phenomenon; research has only begun to scratch the surface of the occurrence of suicide. Under the currently proposed Trump Administration budget, suicide prevention research will receive a budget increase, though the scope and amount of funding is still unclear. While NIH is the current leading authority of suicide prevention research, there exists potential for VA to take a larger leadership role. Increased funding granted by Congress to VA to empirically study suicide could provide new methods of suicide prevention that could be applied to both veterans and the overall U.S. population. Additionally, increased funding would cut down on the time needed to verify and publish data on recent suicide rates, which would provide more dynamic research on trends.
The second area of reform must focus on eliminating the stigma attached to mental health care within the active-duty and veteran military communities. Behaviors that influence and reinforce this stigma are learned through active-duty service and persist after separating from the military. In order to create a positive attitude regarding mental health, the DoD must have every level of leadership create an open dialogue with their subordinates about topics such as mental health, personal issues, and negative behaviors. This open dialogue must be personal and come without fear of retribution or embarrassment to the service member. Service members must also be encouraged to treat their mental health as seriously as their physical health and seek out help for any mental imbalance.
VA will have to take a different approach towards eliminating the military stigma around mental health among those who have already separated from the military. Public media campaigns promoting the benefits of mental health and equating mental health with strength rather than weakness will encourage veterans to be more open to discussing potential mental imbalance. This style of communication concerns the third major area in need of reform: outreach. VA must drastically increase its funding to implement various methods of outreach through social media, advertisements, and events that target younger veterans at higher risk for suicide. The rate of programs and funding for veteran outreach must surpass the 2016 peak and create innovative new methods of connecting with all former service members. VA uses traditional methods of advertisements such as daytime television to attract older veterans with a higher need for medical services, but younger veterans are harder to market to. The effectiveness of outreach efforts is well documented to reduce isolation as well as feelings of thwarted belongingness and perceived burdensomeness, the two constructs of the IPTS.
Staffing is also an area of concern, though recent measures by VA and the Trump Administration seem promising to reducing vacancies at VA hospitals. By adopting measures that provide incentives to medical professionals such as student loan reimbursement, the federal government can expand its ranks of qualified individuals who are invested in their career with VA. Staffing is a perpetual issue with high importance, so it is vital that oversight be conducted on hiring practices by government agencies such as the Office of the Inspector General and the Government Accountability Office.
The final area of concern, and potentially the most complex, involves access to lethal means among veterans. This topic is complicated because gun ownership is not only popular within the veteran population, but also the overall U.S. population. Legislative measures that are even perceived as infringing upon the rights of Americans to own firearms are a politically controversial issue. Unfortunately, stricter gun control measures are needed to reduce their availability to veterans at increased risk of suicide. Firearms present a veteran in mental crisis with an immediate and highly lethal means of carrying out suicide. If VA were to adequately identify veterans owning firearms, it could be cross referenced with patient records to identify individuals in need of intervention. VA could also promote the use of gun locks or gun safes to store their firearms. Barrier methods as simple as a combination code have been known to be positive deterrents that cause veterans in crisis to rethink their actions.
In the broader scheme of American politics, gun control legislative measures would provide intrinsic benefits to veterans. Congress must appropriate significant funding to gun violence research in order to make informed and evidence-based gun control measures. Such gun control measures must directly address the risk that firearm availability presents to anyone suffering from a psychiatric condition or experiencing mental instability. Expanded background checks, investment into new strategies to reduce rates of gun ownership, and Extreme Risk Protection Orders (ERPO) are all viable avenues available to legislators in Congress.
Suicide rates among veterans of the United States military remain a high-priority issue for the Department of Veterans Affairs (VA). Since 2007, there has been over 6,000 suicide deaths in the veteran community annually, an average of approximately 16 to 17 per day [1]. In response to this crisis, VA has implemented new policies and programs aimed at preventing suicides among veterans. However, these initiatives have failed to make any meaningful impact suicide rate despite increases to funding for mental health by Congress. This paper will examine the occurrence of suicide and the factors that put veterans at heightened risk over the nonveteran community. The impact of Congressional legislation on VA policy and funding will also be considered. This paper will also discuss VA’s response to the crisis, where it has fallen short, and finally, what improvements can be made to reduce the rate of suicide among veterans.
Common Acronyms
AFSP- American Foundation for Suicide Prevention
AI/AN- American Indian/Alaska Native
AMVETS- American Veterans
DAV- Disabled American Veterans
DoD- Department of Defense
ERPO- Extreme Risk Protection Order
GAO- Government Accountability Office
IAVA- Iraq and Afghanistan Veterans of America
IPTS- Interpersonal Theory of Suicide
NIH- National Institute of Health
OEF- Operation Enduring Freedom
OIF- Operation Iraqi Freedom
OIG- Office of the Inspector General
PTSD- Post-Traumatic Stress Disorder
TBI- Traumatic Brain Injury
VA- Department of Veterans Affairs
VCL- Veteran’s Crisis Line
VHA- Veterans Health Administration
VSO- Veteran’s Service Organizations
Introduction
Suicide is a phenomenon that has become all too familiar to members of the veteran community in the United States. When adjusted for age and sex, veterans die by suicide at 1.5 times the rate of non-veteran adults within the U.S.. Military personnel and veterans display several noticeable factors that put them at increased risk of suicide over civilians. Despite suicide prevention measures that have been implemented through federal programs, the rate of suicide death among veterans has shown no visible signs of decreasing.
The Department of Veterans Affairs (VA) is the agency responsible for the health care and wellbeing of veterans in the U.S. Over the past decade VA has instituted suicide prevention programs such as the Veteran’s Crisis Line (VCL) for veterans who are currently contemplating suicide and want to speak with licensed specialists. However, VA has faced strong criticism by lawmakers and veteran’s service organizations (VSO) who claim the organization is not taking a proactive approach in reducing the rate of suicide.
This paper will discuss the occurrence of suicide among U.S. veterans, such as what factors put them at increased risk and what methods have been proven to reduce the incidence of suicide. It will also discuss what measures VA, Department of Defense (DoD), and Congress have taken to reduce the rate of suicide as well as whether they have been effective or not. Finally, this paper will make recommendations on how VA can take a more proactive approach to reducing the rate of suicide among veterans.
The Phenomenon of Suicide
Suicide is defined the act or an instance of taking one’s own life voluntarily and intentionally. In 2018, 48,344 Americans died by suicide, making it the tenth-leading cause of death overall in the U.S.. Suicide is a growing problem within the U.S.; from 1999 to 2007 the rate of suicide death among the general U.S. population has increased 33 percent, from 10.5 to 14 per 100,000 people respectively. It is important to note that there is no single cause of suicide. Rather, suicidal ideation (the desire to die by suicide) stems from health, genetic, historical, and environmental stressors that can affect anyone at any period in their lives. Mental health stressors such as depression, substance abuse disorder, post-traumatic stress disorder (PTSD), and traumatic brain injury (TBI) are factors most commonly attributed to successful suicides. Despite its prominence as a national health concern, the act of suicide is still not a well understood phenomenon and preventative measures to reduce suicide rates are still an imperfect science with much room for improvement.
Warning Signs of Suicide
*Incomplete*
Health Factors of Suicide
Depression
Depression is a common but serious mood disorder that causes severe symptoms that affect how one feels, thinks, and handles daily activities such as sleeping, eating, and working. Depression can manifest itself in a number of ways including (but not limited to): persistent sadness/anxiety, feelings of hopelessness or pessimism, irritability, feelings of worthlessness or helplessness, loss of interest in hobbies, difficulty concentrating, and decreased energy or fatigue. Although the majority of people who have depression do not die by suicide, having major depression does increase suicide risk compared to people without depression. The Department of Health and Human Services has estimated that approximately 60 percent of people in the U.S. who die by suicide have a mood disorder such as major depression or bipolar disorder.
Substance Use Disorder/ Alcohol Use Disorder
Substance use disorders (SUD), particularly alcohol use disorder (AUD), influence suicidal behaviors and are linked to a substantial number of suicides and suicide attempts. The Substance Abuse and Mental Health Services Administration (SAMHSA) found in 2014 that approximately 1 in 12 individuals in the U.S. suffered from a substance abuse disorder in the past year and almost a quarter engaged in binge drinking within the last month. A study conducted by the Centers for Disease Control and Prevention (CDC) in 2010 found 22 percent of deaths by suicide involved alcohol intoxication at or above the legal limit. Similarly, acute alcohol intoxication was also present in about 30-40 percent of suicide attempts. Additionally, opiates were present in 20 percent of suicide deaths, marijuana in 10.2 percent, cocaine in 4.6 percent, and amphetamines in 3.4 percent. One reason alcohol and/or drug misuse significantly affects suicide rates in the disinhibition that occurs when a person is intoxicated. Alcohol abuse is also known to increase depressed moods and its availability makes it a prominent concern among suicide prevention researchers.
Post-Traumatic Stress Disorder
Post-traumatic stress disorder (PTSD) is a disorder that develops in some people who have experienced a shocking, scary, or dangerous event. It is natural to feel afraid during and after a traumatic situation, yet people who develop PTSD may continue to feel stressed or frightened, even when they are not in danger. PTSD is a disorder frequently associated with war veterans, however, anyone at any age can develop PTSD; symptoms of PTSD may manifest within three months of the traumatic incident but may sometimes begin years later. Trauma exposure and PTSD are well-established risk factors for suicidal thoughts and behaviors, with research indicating that comorbid [simultaneously present diseases or medical conditions] depression amplifies this risk. Because PTSD is one of the few psychological conditions that predict suicidal behavior among those who think about suicide, many patients with PTSD present clinically with elevate suicide risk.
Traumatic Brain Injury
Traumatic brain injury (TBI) is a sudden injury, such as a blow, bump, or jolt to the head that causes damage to the brain. The main causes of TBI are falls, vehicles crashes, sports injuries, child abuse, or blast injuries due to explosions. Penetrating TBI occurs when an object, such as a bullet or bone fragments from a skull fracture, enters the brain. Symptoms of TBI can be mild, such as a concussion; moderate; or severe. Most people completely recover from TBI, but severe cases can lead to serious psychical and psychological symptoms. Individuals with a history of TBI have been shown to have higher rates of nonfatal deliberate self-harm, suicide, and all-cause mortality than members of the general population. A study conducted over the course of 35 years in Denmark found those with medical contact for TBI compared to the general population without TBI had an increased risk of suicide with an incident rate ratio of 1.9:1[nearly twice as likely to die by suicide]. Additional analyses revealed that the risk of suicide was higher for individuals with severe TBI, numerous medical contacts, and longer hospital stays. The same study found that individuals were at the highest risk of suicide in the first six months after discharge.
Environmental Factors
*Incomplete* Economy and income, unemployment, relationship status, access to firearms
Historical Factors
*Incomplete* Prior suicide attempts, history of family violence/suicide, childhood abuse, neglect, trauma
Why are Veterans at Higher Risk of Suicide?
Suicide is an issue that, in general, affects veterans to a greater degree than non-veterans. The 2019 National Veteran Suicide Prevention (NVSP) Annual Report found that of the 45,390 American adults that committed suicide in 2017, 6,139 were veterans. By these metrics, 13.5% of the total suicide deaths were by veterans, despite the fact that veterans only make up 7.6% of the total population. Since 2007, the age-and-sex-adjusted suicide rate among veterans has increased from 18.5 per 100,000 to 27.7 per 100,000 in 2017. This increase in suicide deaths have occurred despite the fact that during this ten year period the total veteran population decreased by 18.3%. In comparison, the age-and-sex-adjusted suicide rate for the overall U.S. population in 2017 was 18.0 per 100,000 and the population grew by 17% during the same 10 year period.
There is no all-encompassing reason why a veteran would choose to die by suicide; rather, suicidal ideation and risk come from a variety of factors. Veterans who have recently separated from the military may be at risk of suicide due to the loss of camaraderie, the feeling of having no purpose, and a lack of fear or indifference towards death. Longer and more frequent deployments during the armed conflicts in Iraq and Afghanistan have taken a toll on younger veterans, as well as the stress related to combat devices such as improvised explosive devices and suicide bombers. Combat veterans are more likely to suffer from psychiatric disorders such as PTSD, depression, traumatic brain injury (TBI), bipolar disorder, substance abuse, and schizophrenia than those who did not experience combat and non-veterans. Approximately 25% of the total veteran population seen at VA hospital in 2010 reported suffering from at least one of these mental disorders. Additionally, 58.7% of veterans with recent VHA use who died by suicide in 2017 had a diagnosed mental health or substance use disorder.
The most common demographics at risk of suicide in the U.S. overall population are the same demographics that most commonly join the military: white, male, 18-34, and single. The 18-34 age bracket also has the highest rate of suicide in the veteran community at a rate of 45 per 100,000. It is important to note that while white men still comprise the majority of the military and veteran community, demographics are shifting as more minorities and women enlist. For most age groups, men have higher rates of use or dependence on illicit drugs and alcohol than women, though women are as likely as men to develop a substance abuse disorder.
Women Veterans
*Retool and rework entire section*
Access to Firearms
Access to firearms has been proven to increase the likelihood of suicide and nearly 70% of all veteran suicides are committed by firearms. Suicide attempts involving firearms are a particularly lethal means of self-harm, with a fatality rate of approximately 90%. However, gun ownership is incredibly popular in the military; nearly half of all veterans own one or more firearms. For this reason there has never been a concentrated effort to reduce the ownership of firearms by veterans who may be suffering from mental balance issues. Though clear links exist between firearm ownership and suicide risk, there has been a 20 year freeze on gun violence research in the U.S., which has resulted in a lack of empirical evidence. This 20 year freeze was recently ended in December, 2019, but only $25 million was dedicated as part of a $1.4 trillion deal signed by President Trump.
Military Stigma
Mental imbalance and suicidal ideation are significant risk factors of suicide that are not widely discussed within the military and veteran communities. The reluctance to share concerns about one’s own mental wellbeing is linked to a military culture that stigmatizes mental health care. Military culture prides itself on strength, and to admit mental distress is seen as a weakness that should be ignored. This is evidenced by the fact that 43% of veterans who died by suicide did not seek help from military treatment facilities or suicide hotlines in the month before their deaths. Suppression and avoidance of any instability, whether physical or mental, is a tactic taught in the military because, in the short term, they are powerful tools for adapting to the extreme adversity of combat. However, the concept that admitting pain makes one weak has consequences on veteran’s psyche long after they separate from the military, including not reaching out to mental health coordinators when experiencing mental instability.
Another aspect of military stigma that affects service members and veterans is the belief that pursuing mental health care could pose risks to one’s career or a fear of retribution. A common misconception among military communities is that seeking out mental health care of any kind could put their career at jeopardy or could cause their security clearance to be revoked. While it is true that certain psychological conditions could be grounds to revoke security clearance, a past or present mental, emotional, or personality disorder is not by itself a disqualifying condition to hold a security clearance. Likewise, speaking with mental health care professionals and participating in therapy are not disqualifying factors for a security clearance. The security concern arises when the possibility of future unreliable or dysfunctional behavior that could result in the willful or negligent compromise of classified information.
As attitudes towards mental health conditions have shifted towards acceptance in the mainstream consciousness, there has been a concerted effort by DoD and VA to dispel the stigma surrounding mental health care in the military. Military leaders have begun adopting tactics like discussing their own history with mental health conditions, promoting the belief that seeking help is a sign of strength, and educating service members on how to access mental health care. For this change in mindset to truly change the perception surrounding mental health, leaders from the top of the military to the bottom must be willing to change the way they acknowledge pain and suffering. There exists no empirical evidence that such a change in mindset would have an effect of the preparedness and training of the U.S. fighting forces.
Interpersonal Theory of Suicide
The Interpersonal Theory of Suicide (IPTS) proposes that the most dangerous form of suicidal desire is caused by the simultaneous presence of two interpersonal constructs- thwarted belongingness and perceived burdensomeness (and hopelessness about these states)- and further, that the capability to engage in suicidal behavior is separate from the desire to engage in suicidal behavior. Thwarted belongingness is comprised of a sense of isolation and a lack of meaningful and reciprocal relationships; perceived burdensomeness is comprised of self-hatred and a sense that others would benefit from one’s death more so than one’s continued life.
The concepts of thwarted belongingness and perceived burdensomeness are particularly relevant for veterans that have recently separated from the military. The life of a service member revolves around the concept of protecting the U.S. population and the freedoms it espouses; the importance of defending those interests is endlessly impressed upon every service member. Once the service member separates from that highly regimented lifestyle, the belongingness they felt of being a part of something bigger is stripped away and can weigh heavily on veterans. They quickly lose their existing support network of fellow service members and return to an area they have not lived in for a number of years. This sudden shift commonly results in veterans feeling alone and can spiral into isolation if left untreated, a common symptom of suicidal ideation.
The capability for suicide is comprised of an elevated tolerance for physical pain and a diminished fear of death and bodily harm. While genetics play a part in the capability for suicide, it is largely thought to emerge through repeated exposure to painful and/or provocative events, which lead to habituation to stimuli (e.g., pain, impending death) that would otherwise be highly aversive and serve as obstacles to suicidal behavior. The tolerance for any sort of pain is instilled on service members from the moment they begin initial training. In order to be successful in combat, one must learn to ignore pain and keep fighting until the enemy is defeated; this tenet is exemplified in the popular military ethos “train as you fight.” Service members must overcome pain quietly or risk being ridiculed as weak. While the American military approach of neglecting pain is effective in combat, it can have devastating consequences on veterans suffering from mental imbalance.
The Family Unit
The family unit can increase feelings of thwarted belongingness and perceived burdensomeness on veterans returning from deployment. Combat and non-combat deployments cause a great deal of stress on families of those deployed, and this stress likely contributes to family problems that arise during and after deployment. Stress within families does not end when the service member returns home from a deployment. Over 75% of married service members report some family readjustment issue post-deployment, with 66.6% reporting one or more concerns occurring on a weekly basis. Readjustment issues such as feeling like a guest in their own home, children being cold toward them, being unsure of responsibilities in the home, and intimacy issues are problems commonly reported in service members that return with any level of depression, PTSD, or generalized anxiety disorders.
Perceived burdensomeness is a significant risk for veterans with young children. Within the families of deployed service members, studies have found links between parental deployment and behavioral and academic problems in children, as well as child maltreatment and intimate spousal abuse. During long periods of absence, the deployed parent will inevitably miss milestones in their children’s development. It is not uncommon for children in these circumstances to not remember the deployed parent or may even be afraid of them. This can increase the anxiety on already struggling veterans and contribute to feelings of being a stranger within their own home. Feelings of being a stranger in the veteran’s own home can be compounded by the delegation of responsibilities with their spouse. After a 7-12 month deployment, service members return home and may be tempted to rush to return to the pre-deployment “normal.” During that absence the spouse has stepped up to handle all household and child-raising responsibilities. After doing things their way for so long, the spouse may be reluctant to relinquish control.
Suicide Rates Between Veterans and Non-veterans *Appendix A*
Veterans are not the only demographic who have seen an increase in suicide rates within the United States. Appendix A shows that between 1999 and 2018 the suicide rate increased by 35%, from 10.5 per 100,000 to 14.2 for a total of 48,344 deaths and an estimated 1.4 million suicide attempts in 2018. It is important to note during this timeframe the suicide rate increased by a rate of .8% per year from 1999 to 2006, and increased to 2.1% per year from 2006 to 2018. The increasing rate of suicide has made it the tenth-leading cause of death for all ages in the U.S., though it is the second-leading cause of death for those between 10-34 years old. To determine which groups are most at risk, the total suicide count can be broken down by four criteria: sex, age, race, and location.
Sex *Reference Appendix* *Appendix B*
The rate of suicide deaths by males comprises the majority of total suicide deaths; males are 3.5 times more likely than women to die by suicide on average. Between 1999 and 2018 the rate of suicide deaths by males rose 28%, from a rate of 17.8 in 1999 to 22.8 in 2018. During this same time period the rate of suicide deaths among women rose from 4.0 in 1999 to 6.2 in 2018 for an increase of 55%. As of 2017, males represent 79% of all U.S. suicides even though women attempt suicide three times as often as males. The reason for this imbalance can be linked to the method of suicide; firearms are the most common method used by males and are highly lethal, while females most commonly use less lethal means such as ingesting poison and suffocation.
There are direct correlations between the trends of suicide by sex between the nonveteran and veteran populations in the U.S. For instance, males die by suicide at much higher rates than women in both populations. Males are also more likely to use highly lethal means such as firearms, while women more frequently use less lethal means such as poisoning and suffocation. However, males and women veterans differ from their civilian counterparts regarding firearm suicide; both sexes in the veteran community are more likely to use firearms when dying by suicide. Additionally, women veterans die by suicide at a much higher rate (15.9 per 100,000) than nonveteran women, making it difficult to draw deeper inferences between the two populations.
Age *Appendix C*
Among the age brackets of 10-14, 15-24, and 25-34 suicide is the second-leading cause of death for an average of 16.74 per 100,000. However, broken down by age, the 55-64 age bracket has the highest incidence of suicide at 20.2 per 100,000 as of 2018, narrowly rising above the 45-54 age bracket where the rate of suicide is 20.04 per 100,000. According to the American Foundation for Suicide Prevention, younger groups have had consistently lower suicide rates than middle-aged and older adults. The incidence of suicide by age group in the nonveteran population does not show a correlation with the veteran population, where suicide rates are highest in the 18-34 age groups at a rate of 44.5 per 100,000.
Race *Appendix D*
In the U.S., White people die by suicide at rates much higher than any other race barring American Indians/Alaska Natives (AI/AN); White people also make up the majority of the U.S. population as well as the military and veteran community. In the medical community, there are several theories that may explain why White people die by suicide so frequently, but none are conclusive. The most frequently noted theory points to the ongoing opioid epidemic which largely affects white, rural communities.
Though they only make up 1.3% of the U.S. population, American Indian and Alaskan Natives have the highest rate of suicide among all ethnic groups in the country. According to the CDC these two indigenous populations die by suicide at a rate of 22.4 deaths per 100,000. Among the AI/AN veteran community the rate is even higher at 31.5 deaths per 100,000. In comparison, the rate of suicide among Black, Asian, and Hispanic nonveteran populations ranges from 6.9-7.1 per 100,000. The high incidence of suicide in AI/AN communities can be linked to existing health and societal disparities that negatively impact indigenous tribes in the U.S. Chief among these disparities is a lack of access to mental health care such as psychiatrists and psychologists. Alcohol abuse and untreated depression are high among AI/AN populations due to poor economic opportunities on reservations; autopsies performed on AI/AN suicides were much more likely to test positive for marijuana, alcohol, or amphetamines than White suicides.
There is a correlation between the rate of suicide by race in the nonveteran and veteran population of the U.S. White people and AI/AN people have far higher rates of suicide than Black, Hispanic, and Asian populations. Though there are culturally significant issues that must be noted, such as alcoholism among AI/AN people and opioid abuse among White people, geographic location may also play an important role. AI/AN communities are more likely to be rural if they are living within a reservation. Additionally, White people make up 77.8% of the total population living in rural communities in the U.S.. Geographic location and its impact on suicide rates will be explored in the next section.
Location *Appendix E*
The occurrence of suicide is much higher in rural Southern and Midwestern areas than in heavily developed and urban states in the Northeast and West. There are a number of contributing factors that explain this discrepancy. As previously stated, mental health services such as psychiatrists, psychologists and pharmacies can be scarce or non-existent in rural communities. Rural communities suffer from a shortage of mental health care professionals that are able to reside in each community which leads to long wait-times. Rural communities also tend to be spread out over large distances, creating many small and close-knit communities. Rural residents wishing to receive mental health care may sometimes have to travel hours to the nearest population center to receive care and may be forced to pay out of pocket for treatment when they do. Due to the close-knit nature of these small towns, lack of anonymity can also be a barrier to treatment out of fear of embarrassment or fear.
Rural communities also suffer from a similar mental health stigma that the military and veteran communities do. The fear of embarrassment or being labeled ‘crazy’ by one’s neighbors can be a powerful deterrent to seeking mental health care. The lack of anonymity in a small town may also cause fear of gossip amongst neighbors, though in general individuals in rural communities are similar to urban communities that they contribute neither positive or negative characteristics to a personal with depressive symptoms. Like the veteran community, individuals in rural areas may be less willing to admit the existence of depressive symptoms out of fear of the stigma they perceive is attached to mental health, despite evidence showing such a stigma is not attached to mental health care.
Conclusions on Nonveteran Suicide Statistics
There are many correlations between suicides in the nonveteran population and veteran population. White people have the second highest rate of suicide in the U.S. and have the highest rate of suicide in the veteran community. While AI/AN people have comparable rates of suicide, they make up a much smaller segment of the country, meaning the vast majority of suicide deaths in the U.S. are attributed to white people. Within the White population, there is large discrepancy regarding the rate of suicide between White males and White females; men of every ethnicity have much higher rates of suicide than women. The veteran community follows the same trend; White males make up the majority of suicide deaths. However, within the military and veteran community White males are disproportionately represented in comparison to the greater U.S. population by a wide margin. Up to a quarter of all White male veterans come from rural areas of the country that are often higher in poverty rates and lower in education rates than more developed areas of the country. When veterans return home to these rural areas, they may experience a lack of employment opportunities and appropriate health care relating to depression of suicidal ideation.
Suicide Prevention Methods
Psychotherapy, Outreach, Medication, Alternative therapies
USI Preventative Model (Not yet written)
Congressional Response to Elevated Veteran Suicide Rates
The responsibility for funding to VA and all mental health legislation falls on the two chambers of the U.S. Congress. Due to veteran’s status as a universally sympathetic group, veteran mental health is a perpetual high-priority target for legislation. Veterans are also a highly visible group; stories of veterans suffering with disability or dying by suicide elicit strong emotional reactions among the voting population that puts pressure on Congress to act. Both chambers of Congress have a Committee on Veterans Affairs where most legislation originates. However, legislators representing veteran-heavy districts may propose legislation based on dialogue with veterans in their constituency.
*New section on process taken to craft legislation focused on veteran suicide, including both chamber Committees/Subcommittees, lobbying by VSO’s, Congressional hearings? (could explain the emotional factor and contain it to one section)*
Joshua Omvig Veterans Suicide Prevention Act of 2007
Specialist Joshua Omvig was a soldier in the U.S. Army who died by suicide shortly after returning from an 11-month deployment to Iraq in 2004. A posthumous profile piece in Omvig’s hometown newspaper detailed the many symptoms of post-combat PTSD the soldier exhibited including nightmares, visible shaking, re-acclimatization issues, and the inability to discuss his experiences. In December of 2005, Omvig was arrested for drunk driving; he died by suicide in his vehicle the next day after being released from jail.
Omvig was far from the only high-profile suicide to occur during this time period. In 2007, Veterans for Common Sense filed suit on behalf of 320,000 to 800,000 veterans or their survivors against then-VA Secretary Jim Nicholson asking for relief in the form of immediate mental health treatment for veterans. In response, Congress drafted several bills ordering VA to take specific measures to improve mental health care for veterans, but none of the proposals made it through committee in either house of Congress. In early 2007, Rep. Leonard Boswell, the Democrat Representative of whom Omvig was a constituent, introduced the Joshua Omvig Veterans Suicide Prevention Act, which was seen as less specific and wide-ranging than previous legislative attempts, but would still require VA to address the problem of veteran suicide. The bill was signed into public law by President George W. Bush with 152 co-sponsors and unanimous votes in both the House and Senate.
The Joshua Omvig Veterans Suicide Prevention Act of 2007 (Omvig Act) is considered to be the first enacted piece of legislation specifically addressing veteran suicide. The Omvig Act (PL 110-110) ordered the Secretary of VA to develop and carry out a comprehensive program designed to reduce the incidence of suicide among veterans that included six specific provisions set forth by Congress. As part of the legislation, the VA Secretary was also required to submit a report within 90 days of the passage of legislation to provide a report to Congress containing information on the status of the implementation of the comprehensive program, the timeline and costs for complete implementation of the program, and a plan for additional programs and activities designed to reduce the occurrence of suicide among veterans.
The first requirement established mandatory training for appropriate staff, contractors, and medical personnel who interact with veterans that included information on recognizing risk factors of suicide, proper protocols for responding to veterans who may be at high risk of suicide, and best practices for suicide prevention. Though the Act did not prescribe a set of best practices, it required VA to conduct research in conjunction with the HHS, NIMH, SAMHSA, and CDC to determine the best practices in veteran suicide prevention.
The second requirement in the Omvig Act requires VA medical staff to offer mental health evaluations in their overall health assessment and to provide referrals (at the veteran’s request) to appropriate counseling and treatment programs for veterans exhibiting symptoms of mental health problems. This provision reduced the barriers frequently encountered by veterans seeking mental health care who did not have a documented mental illness but exhibited symptoms of suicidal ideation.
The Omvig Act also called for the designation of suicide prevention counselors at each VA medical facility. The legislation outlined the role of suicide prevention counselors as one who works with local emergency rooms, police departments, mental health organizations, and veterans service organizations to engage in outreach to veterans and improve the coordination of mental health care to veterans. The establishment of this position allows VA facilities across the country the ability to work with local resources to reach out and provide care to veterans who may not be enrolled in the VA health system but may be experiencing a mental health crisis, including homeless veterans.
The fourth requirement of the Omvig Act called for the VA Secretary to provide research on mental health care for veterans who have experienced sexual trauma while in military service. Military sexual trauma (MST) is a systemic problem within the military; while men do experience MST, the problem is less far-reaching than women veterans who experience MST at much higher rates.
One of the most successful initiatives to come out of the Omvig Act is the establishment of the Veterans Crisis Line (VCL). The VCL is a 24/7 free, anonymous, confidential resource that is available to all veterans, service members, family members, and friends regardless of enrollment in VA. Veterans who contact the VCL speak with qualified responders specially trained and experienced in helping veterans of all ages and circumstances. VCL responders listen to the veteran and, when applicable, provide resources for further care or initiate the dispatch of emergency services to callers in crisis. Since its establishment in 2007 the VCL has handled more than five million calls and has dispatched emergency services to callers in crisis more than 159,000 times. Additionally, VCL has provided more than 897,000 referrals to VA suicide prevention coordinators to make it easier for veterans to receive more permanent assistance. In 2009 the VCL was expanded to support online chats; to date VCL has handled more than 585,000 online chats. In 2011 the VCL was further expanded to support text-message services and has since handled more than 184,000 conversations with veterans who did not wish to speak directly.
The sixth and final requirement of the Omvig Act pertains to outreach and education for veterans and their families with a special emphasis on OIF and OEF veterans. The educational programs created through this provision were designed to remove the stigma associated with mental illness, encourage veterans to seek treatment and assistance for mental illness, and to promote skills for coping with mental illness. Additionally, educational programs were created aimed at helping the families of veterans in understanding the issues arising from the readjustment of veterans to civilian life, identifying the signs and symptoms of mental illness, and encouraging veterans to seek assistance for mental illness.
Though it was not included as a requirement under the comprehensive suicide prevention program, Congress also encouraged the VA Secretary through the Omvig Act to create a volunteer peer support counseling program. From this recommendation, VA created the Peer Support Mentoring Program to link veterans with veteran mentors who have experienced similar challenges and situation. Under the peer support program, veterans are trained to conduct outreach to veterans and their families as well as adequately assist other veterans with issues related to mental health and readjustment. Veteran mentors do not only serve as a friend and a good listener, but also as someone who can provide first-hand experience in navigating the intricacies of the VA health system. The success of the Peer Support Mentoring Program has prompted many prominent VSO’s to create their own version of the program for its members to connect together.
Clay Hunt Suicide Prevention for American Veterans Act
While the Joshua Omvig bill was the first step, the legislation that has led VA to where it is currently is the Clay Hunt Suicide Prevention for American Veterans Act (Clay Hunt SAV Act). The Clay Hunt SAV Act is named for Sgt. Clay Hunt, a Marine sniper who took his life in 2011, just two weeks after seeing a VA psychiatrist. While Joshua Omvig’s story dealt with the effects of undiagnosed PTSD, Clay Hunt’s story focused on VA’s failure to help him when he reached out. Congressional testimony provided by Hunt’s mother highlighted how, despite his pro-active approach to seeking health care, he struggled to get appointments with a psychiatrist and felt like a guinea pig as a variety of medications were tried to treat his PTSD. The Clay Hunt SAV Act represented the chance to make substantial change within VA, a move President Obama was eager for in the wake of the 2014 Phoenix Waiting Room scandal.
The first provision of the Clay Hunt SAV Act established a yearly third-party evaluation of VA’s mental health care and suicide prevention programs. The annual mental health care report uses metrics common among mental health care practitioners and identifies the most effective programs conducted through VA for suicide prevention. The yearly report also provides information on the cost-effectiveness of these programs and evaluates the level of patient satisfaction with respect to their involvement in any VA program. Finally, the report provides systematic updates to and recommendations for best practices regarding veteran mental health and suicide prevention.
The second provision of the Clay Hunt SAV Act required VA to survey the Department’s existing websites and information resources to create a centralized website that serves to provide veterans with information regarding all of the mental health care services provided by VA. In addition to serving as a singular point of information, the Act requires that the website contain information on resources available to veterans within their regional VA network, including the name and contact information of local social work offices, mental health clinics, and a list of appropriate medical staff. The website, mentalhealth.va.gov, has grown since its inception and now provides veterans and their families with a local resource finder, informative pages covering all forms of mental illness, and support resources for specific types of veterans and civilians. The final requirement of this provision ensures all information and sources available through VA’s centralized website are updated and corrected no less than every 90 days or as more current information becomes available.
The third provision called on the VA Secretary to establish a pilot program that repaid the educational loans for certain psychiatrists working for VHA within three years. Under this pilot program, individuals licensed or eligible for licensure to practice psychiatric medicine, as well as those enrolled in the final year of a residency program leading to specialty qualification in psychiatric medicine, would be eligible to have their student loans repaid. Individuals participating in this program would be required to enter into a period of obligated service of two or more years with VHA in the field of psychiatric medicine.
The fourth provision called on the VA Secretary to establish a pilot program to assist veterans transitioning from serving on active duty and to improve the access of veterans to mental health services. Under the pilot program a community oriented veteran peer support network would be established within certain VISN’s to help veterans navigate VA’s resource and benefits system. Additionally, a community outreach team would be created at medical centers with the aim of assisting veterans transitioning into communities, facilitate outreach activities between veterans and their communities, and act as liaisons between veteran and local resources such as legal aid.
The fifth provision of the Clay Hunt SAV Act eliminated bureaucratic red-tape between VA and non-profit mental health organizations to improve the efficiency and effectiveness of suicide prevention efforts. The elimination of bureaucratic barriers allows for trained VA medical professionals to lend their expertise to local suicide prevention non-profits through best practices and collaboration to exchange training sessions between organizations.
The final provision of the Act, included to appease Congress people opposed to government spending, prohibited any new appropriations for the reforms to be implemented within VA. Instead, VA was forced to cannibalize its own budget and pull funding away from other projects to complete requirements such as the centralized website. In the five years since the SAV Act became law, VA has submitted to Congress a yearly report of the pilot programs the Act established. Veteran’s service organizations such as American Veterans (AMVETS) and the Iraq and Afghanistan Veterans of America (IAVA) have provided significant pushback against VA over the findings of the report as well as recommendations on how to address systemic problems in the agency. An IAVA report published in 2019 found that the loan repayment pilot program and the transition assistance pilot program have suffered from a lag in funding because no additional funds were allocated to VA by Congress. The same report found that increases in funding for mental health care through the Trump Administration budget have recently allowed these programs to get underway.
Choice Act
During the same time period as the Clay Hunt SAV Act, feelings of frustration in the public over veteran health care were exacerbated by outrage over the 2014 “Waiting List” scandal. In April 2014, a CNN investigative report found that hospital directors at a Phoenix, Arizona VA hospital were keeping secret waiting lists of veterans seeking appointments with their primary care physician. These waiting lists were hidden from federal regulators to produce lower average wait metrics, which resulted in the potentially preventable deaths of at least 35 veterans. The public outcry over the scandal eventually led to the resignation of VA Secretary Eric Shinseki and amplified calls for reform within the organization.
From this scandal, the Veterans’ Access to Care through Choice, Accountability, and Transparency Act of 2014 (Choice Act) was signed into law by President Obama on 7 August, 2014. The Choice Act provided veterans with the option to get non-VA health care from community providers paid for by VA if they live more than 40 miles from a VA medical facility or if they must wait more than 30 days to receive an appointment at VA hospitals. While it was not mental health-specific in nature, the Choice Act gave veterans options outside VA where they could receive health care and mental health care. Additionally, the Choice Act dedicated $500 million in funding to hire more doctors and nurses at VA hospitals, which helped to reduce staffing shortages and lagging pay scales among employees. The Choice Act ran out of funding in May 2018 and was replaced by an expanded version of the program, named the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks Act of 2018 (MISSION Act), signed into law by President Trump in June 2018.
MISSION Act
Under the MISSION Act, the Choice program was expanded to consolidate community care programs, create better customer service, provide new urgent care benefits, and modernized IT systems within VA. The MISSION Act also altered the distance requirements to use the Choice program, changing it from a 30 mile distance to a 30 minute average drive for primary care, mental health, and non-institutional extended care services. The MISSION Act was implemented on June 6, 2019, though it is too early to conduct a thorough analysis.
Commander Scott Hannon Veterans Mental Health Care Improvement Act
The Commander Scott Hannon Veterans Mental Health Care Improvement Act (S. 785) was passed by both chambers of Congress on September 25, 2020. The bill will now travel to the desk of President Trump, who is expected to sign the legislation into law. The Hannon Act gained the support of the White House, VA, dozens of veteran’s service organizations, and Republican and Democratic lawmakers. The legislation, considered by Senator Jerry Moran to be the most significant bill regarding veteran’s mental health care to come out of the committee. The Hannon Act will provide funding for increased research into mental health problems, and will consider a number of nontraditional therapy methods, including hyperbaric oxygen therapy, animal therapy, agritherapy, and art therapy among others.
The Hannon Act will also provide critical funding to increase staffing in VA hospitals and will introduce a pilot program to provide grants for those working at vet centers across the country. An important piece of the legislation will also create independent oversight on VA’s outreach campaign, which has seen far less engagement in the past two years than at its peak in 2016. One other notable portion of the Hannon Act includes legislation specifically relating to women veterans. Under the legislation VA must create a centralized website for women veterans to access all benefits and resources that apply to them, including counseling for MST.
Veterans Affairs
The Department of Veterans Affairs is the federal executive branch that oversees all issues pertaining to veterans and their health care. VA is comprised of three separate administrations: the Veterans Health Administration, Veterans Benefits Administration, and the National Cemetery Administration. The Cabinet-level organization is headed by the Secretary of Veterans Affairs, a position chosen by the president and confirmed through vote in the Senate. The current Secretary of Veterans Affairs, Robert Wilkie, was nominated by President Trump and confirmed in the Senate in July 2018.
Of the three organizations comprising the VA, the Veterans Health Administration (VHA) oversees veteran health care, research and the training of physicians through affiliations with educational institutions. VHA serves over 9 million enrolled veterans annually at 1,255 health care facilities. The responsibility of addressing and reducing the incidence of veteran suicide falls on VHA. Where funding is concerned, VA and DoD combined are the third largest research authorities on suicide prevention, behind NIH and the American Foundation for Suicide Prevention (AFSP) (NAASP 12). Primary oversight for VHA is provided by VA’s executive branch, the Government Accountability Office (GAO), the Inspector General of Veterans Affairs, and the House and Senate Committees on Veterans Affairs.
New Regulations and Legislation Implementation
The rules and regulations of VA and VHA are constantly changing as new research is conducted and “best practices” standards evolve. In the VA Executive Office, the Office of Regulation Policy and Management is responsible for the formulation and control of all VA regulations. The Office of Regulation Policy and Management provides a centralized management and control structure that reports directly to the Secretary and Deputy Secretary of Veterans Affairs. Among areas under its purview, the Office conducts comprehensive overview, reorganization, and rewriting of VA’s existing regulations; it also works with the Office of Congressional and Legislative Affairs to implement new legislation and initiatives such as pilot programs.
The Office of Congressional and Legislative Affairs is the focal point for VA management and coordination of all matters involving Congress. The two offices work together under the direction of the VA Secretary to create pilot programs authorized through enacted Congressional legislation to explore new methods of treating veteran mental illnesses. Pilot programs conducted at individual VA hospitals that demonstrate positive results are referred back to the Office of Regulation Policy and Management to be implemented across all VA hospitals and outpatient facilities.
Criticism of Veterans Affairs
Due to its nature as a highly visible Cabinet-level department, VA has received significant scrutiny by veterans, VSOs, the news media, Congress, and government oversight organizations. Criticism of VA tends to revolve around certain topics: struggles with staffing, wait times, funding, information systems such as electronic medicals records, gender and minority health care disparities, and lack of uniform standards enforced at individual hospitals. While VA has committed itself in recent years to addressing these systemic failures, the process has experienced setbacks as well as successes.
One of the core issues affecting reform within VA is funding. Pilot programs for new methods of treating veterans and attracting staff have not received adequate funding, which has led to delays in implementation and results. The issue of funding may not be that it is inadequate, but rather that funds appropriated to VA have a too-narrow scope. Congress appropriates VA’s budget as a nondefense discretionary program, thus, Congressional priorities can influence both the level of money available and the way VA may spend the money once allocated. For example, programs in VA may be left underfunded despite the availability of excess funds in other initiatives because those funds have been specifically earmarked by Congress. This level of bureaucratic red-tape is typical of any large agency, but it has stymied the organization from making much needed reforms. Since 2016 there has been a concerted effort to cut red tape by eliminating outdated VA policies and streamlining the funding process.
Staffing at VA hospitals is another area where VHA receives continuing criticism. This issue affects every level of VA, from nurses in rural VA locations to Medical Directors managing entire VA hospitals. An OIG report released September 2019 found 96% of VHA facilities reported at least one severe occupational shortage, 39% of which noted at least 20 severe occupational staffing shortages. The same OIG report found that VA has difficulty hiring Medical Directors to hospital due to the high stress of the position, a salary lower than the private sector, unclear recruiting processes, and career risk due to negative publicity. Having high turnover rates and vacancies in the highest position in a VA hospital exacerbate issues like uneven standards of care and wait times that cause the organization to draw such negative attention.
Despite updates to pay scales for VA hospital workers, nearly 40,000 of the 335,000 positions in the Veterans Health Administration are still vacant. The majority of these vacancies reside in densely populated areas such as Los Angeles, California and deeply rural states like Montana and Colorado. Historically lower pay scales have made it difficult to attract medical professionals to less populated areas, which can increase wait times or make some services unavailable in particular areas. Fortunately, there has been improvement in this area under the MISSION Act, signed by President Trump, which increases pay scales to make VA positions more attractive. Pilot programs such as the student loan repayment program for psychiatric medicine graduates have the potential to fill these vacancies if they are implemented through the entire VA organization. This pilot program is currently ongoing and its feasibility has not yet been established.
The Trump Administration
Under the Trump Administration, VA has been marked by record turnovers and vacancies of leadership that have had negative effects on the agency. Over the past five years, VA has had four different Secretaries and four more acting Secretaries. Additionally, VA’s top health official post, Under Secretary for Veterans Health Administration, has been vacant since President Trump took office. The most recent example of turmoil in VA leadership under President Trump came when VA’s second ranking official, Deputy Secretary of Veterans Affairs James Byrne, was abruptly removed from office after just five months in the position. Byrne was dismissed by Secretary of Veterans Affairs Robert Wilkie, who declined to give any reason for the removal outside a ‘loss of confidence.’
These abrupt changes in leadership are having a direct effect on VA’s ability to provide mental health care to veterans at risk of suicide. The lack of consistency among leadership and the vacancies of top positions were highlighted in a 2018 GAO report that found senior leadership has lacked the stability needed to ensure issues policy meets agenda goals. The report shows funding for outreach content for social media had been increasing from 2013 until it peaked in 2016. After the 2016 peak, that outreach declined steeply, and was on track to be below 2013 levels by 2018. Research has shown that outreach programs are effective in preventing suicide; reducing outreach could increase feelings of loneliness among veterans. Outreach by VA is vital to the mission of suicide prevention; as many as 52% of veterans are not enrolled in VA or VHA. When a veteran sees an advertisement or public safety announcement regarding their mental health, they may remember they are not alone and reach out to VA or VCL for help.
On June 17, 2020, President Trump unveiled the President’s Roadmap to Empower Veterans and End a National Tragedy of Suicide (PREVENTS). PREVENTS is an interagency task force intended to reduce bureaucratic red-tape and consolidate federal suicide prevention efforts into one comprehensive nationwide strategy. While the PREVENTS task force does not include physical legislation, it does provide a series of recommendations that will be implemented across VA as well as other federal programs. Central to the task force are reforms to how suicide prevention research is conducted. PREVENTS will identify and prioritize suicide surveillance and research that focuses on a veteran’s unique combination of individual, relationship, community, and societal factors to deliver the most effective intervention(s) tailored to meet their needs and circumstances. Additionally, the program will promote foundational changes to the way research is conducted- including improving the speed and accuracy with which research is translated into practice, improving efficiency through data sharing and data curation practices, and using innovative funding techniques to drive team science and reproducibility.
PREVENTS is also intended to reduce bureaucratic red-tape by developing partnerships across government agencies and nongovernment entities and organizations to increase capacity and impact of programs and research to empower veterans and to prevent suicide. These initiatives will be funded through an interagency federal funding mechanism working with suicide prevention programs at both the federal and local level. The PREVENTS task force has practical improvements for suicide prevention programs and research that may benefit veterans by helping VA avoid future bureaucratic constraints that have historically hamstrung the process. Critics of the PREVENTS task force include Senators Jon Tester, Jerry Moran, and Rep. Mark Takano, who claim the initiative does not provide enough concrete steps to legislate policy changes. Rep. Takano stated that PREVENTS amounts to “Tepid calls for more research, interagency coordination and meek public education campaigns won’t do enough to end this crisis,”. While PREVENTS is a White House program, Congressional leaders on the House and Senate Committees on Veterans’ Affairs have promoted the recently Congressionally-passed Commander Scott Hannon Veterans Mental Health Care Improvement Act.
Funding for Suicide Prevention
Suicide is still not a well understood phenomenon and research into the subject has not been adequately funded. The lack of adequate funding for suicide prevention research extends beyond VA and includes civilian research. Despite being the 10 leading cause of death among Americans, research into suicide prevention receives a fraction of funding that other issues do. For example, the National Institute of Health (NIH) found that from the time period of 2008 to 2013, approximately $430 million was dedicated to suicide research. However, in 2016 alone $500 million was spent on alcoholism research and $690 million on breast cancer research. To put that into comparison, 45,000 Americans die by suicide each year and 65,000 die from alcoholism.
The NIH report, “U.S. National Suicide Prevention Research Efforts: 2008-2013 Portfolio Analysis” shows that of the 383 studies done on suicide prevention during this timeframe, the NIH conducted 156 studies, the AFSP conducted 99, and VA/DOD conducted 82 combined. The AFSP hopes to use these studies to establish a system of best practices aimed at drastically reducing the annual rate of suicide by 2025. The initiative, named Project 2025, will create a predictability model to determine which prevention methods could have the greatest impact, and establish benchmarks to measure against for the next 10 years. The four phase program will take those findings and develop specific strategies for reducing the rate of suicide, and collaborate with other suicide and mental health organizations to focus their prevention efforts on the kinds of programs, policies, and interventions that will save the most lives in the shortest amount of time. The associate director of the Center of Excellence for Suicide Prevention within VA sits on the 17-member advisory committee for Project 2025.
How Suicide Prevention Research is Conducted
Research for suicide prevention is conducted through multiple federal agencies every year. In the U.S., three federal agencies conduct the majority of suicide prevention research: NIH, DoD, and VA. Among these agencies, the NIH has the greatest capacity to conduct research into suicide prevention; the DoD is second-highest and is closely followed by VA. While it is not a federal agency, the AFSP funds more research into suicide prevention more than both the DoD and VA through private donations. Smaller public health organizations, such as the Substance Abuse and Mental Health Services Administration and the Brain & Behavioral Research Foundation, also conduct research into suicide prevention, though their studies are smaller in scope than larger federal agencies.
At the surface level, it may seem redundant to have multiple federal agencies all conducting independent research into suicide prevention. However, all federal agencies are funded independently of each other through Congress’ yearly budget and do not compete for resources. Rather, each agency conducts research relevant to the populations they oversee. For instance, studies funded through the NIH pertain to suicide and suicide prevention among the total U.S. populace, of which active-duty military and veterans represent a small percentage. Research studies funded and conducted through VA pertain only to veterans and their immediate family. Likewise, research conducted through the DoD uses active-duty and reserve military as their sample population.
The results of all peer-reviewed studies and research conducted through federal agencies such as the DoD and VA are all published on the PubMed website, run by the NIH, no later than 12 months after results are released. Publishing results of studies under one agency makes it easier for researchers to use previous information gathered from other entities to increase their sample size while cutting out redundant bureaucratic red-tape. The PREVENTS Roadmap unveiled under President Trump seeks use shared information between agencies to create a comprehensive nation-wide suicide prevention program that also includes research conducted by private entities. The goal of sharing results between agencies under the PREVENTS Roadmap will identify biomarkers in active-duty military, veterans, and civilians that will predict suicidal ideation and risk factors among all groups that may otherwise go unnoticed.
Conclusion and Recommendations
Based upon the evidence presented in this report, there are several areas that represent the biggest challenges facing VA in reducing the rate of suicide among veterans. The first area of concern involves the funding appropriated to mental health care research and the number of studies that are conducted. Suicide is still a relatively unknown phenomenon; research has only begun to scratch the surface of the occurrence of suicide. Under the currently proposed Trump Administration budget, suicide prevention research will receive a budget increase, though the scope and amount of funding is still unclear. While NIH is the current leading authority of suicide prevention research, there exists potential for VA to take a larger leadership role. Increased funding granted by Congress to VA to empirically study suicide could provide new methods of suicide prevention that could be applied to both veterans and the overall U.S. population. Additionally, increased funding would cut down on the time needed to verify and publish data on recent suicide rates, which would provide more dynamic research on trends.
The second area of reform must focus on eliminating the stigma attached to mental health care within the active-duty and veteran military communities. Behaviors that influence and reinforce this stigma are learned through active-duty service and persist after separating from the military. In order to create a positive attitude regarding mental health, the DoD must have every level of leadership create an open dialogue with their subordinates about topics such as mental health, personal issues, and negative behaviors. This open dialogue must be personal and come without fear of retribution or embarrassment to the service member. Service members must also be encouraged to treat their mental health as seriously as their physical health and seek out help for any mental imbalance.
VA will have to take a different approach towards eliminating the military stigma around mental health among those who have already separated from the military. Public media campaigns promoting the benefits of mental health and equating mental health with strength rather than weakness will encourage veterans to be more open to discussing potential mental imbalance. This style of communication concerns the third major area in need of reform: outreach. VA must drastically increase its funding to implement various methods of outreach through social media, advertisements, and events that target younger veterans at higher risk for suicide. The rate of programs and funding for veteran outreach must surpass the 2016 peak and create innovative new methods of connecting with all former service members. VA uses traditional methods of advertisements such as daytime television to attract older veterans with a higher need for medical services, but younger veterans are harder to market to. The effectiveness of outreach efforts is well documented to reduce isolation as well as feelings of thwarted belongingness and perceived burdensomeness, the two constructs of the IPTS.
Staffing is also an area of concern, though recent measures by VA and the Trump Administration seem promising to reducing vacancies at VA hospitals. By adopting measures that provide incentives to medical professionals such as student loan reimbursement, the federal government can expand its ranks of qualified individuals who are invested in their career with VA. Staffing is a perpetual issue with high importance, so it is vital that oversight be conducted on hiring practices by government agencies such as the Office of the Inspector General and the Government Accountability Office.
The final area of concern, and potentially the most complex, involves access to lethal means among veterans. This topic is complicated because gun ownership is not only popular within the veteran population, but also the overall U.S. population. Legislative measures that are even perceived as infringing upon the rights of Americans to own firearms are a politically controversial issue. Unfortunately, stricter gun control measures are needed to reduce their availability to veterans at increased risk of suicide. Firearms present a veteran in mental crisis with an immediate and highly lethal means of carrying out suicide. If VA were to adequately identify veterans owning firearms, it could be cross referenced with patient records to identify individuals in need of intervention. VA could also promote the use of gun locks or gun safes to store their firearms. Barrier methods as simple as a combination code have been known to be positive deterrents that cause veterans in crisis to rethink their actions.
In the broader scheme of American politics, gun control legislative measures would provide intrinsic benefits to veterans. Congress must appropriate significant funding to gun violence research in order to make informed and evidence-based gun control measures. Such gun control measures must directly address the risk that firearm availability presents to anyone suffering from a psychiatric condition or experiencing mental instability. Expanded background checks, investment into new strategies to reduce rates of gun ownership, and Extreme Risk Protection Orders (ERPO) are all viable avenues available to legislators in Congress.
Appendix A- General
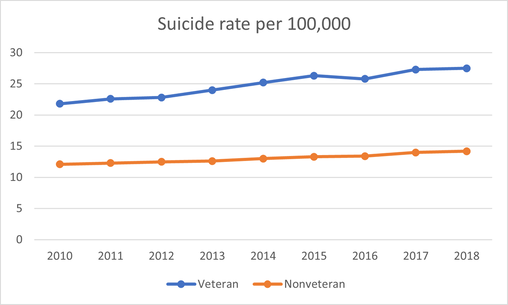
Appendix B- Sex
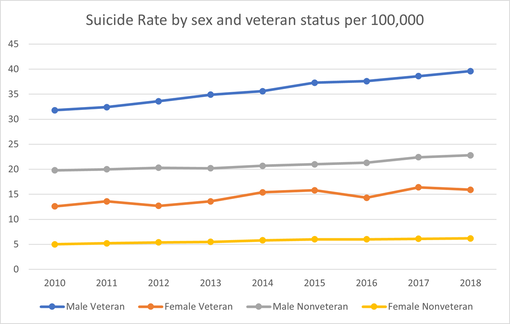
Appendix C- Age
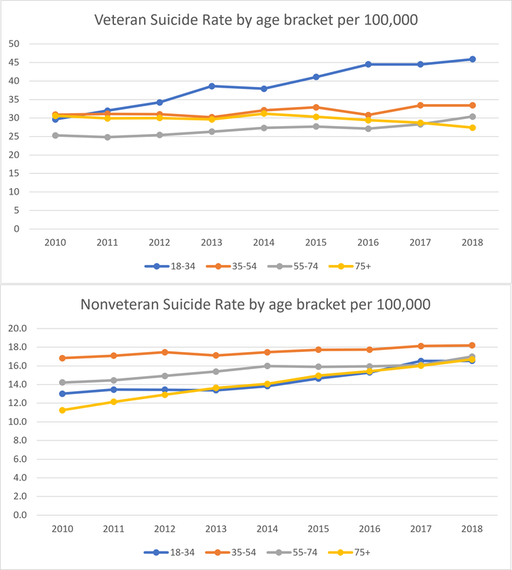
Appendix D- Race
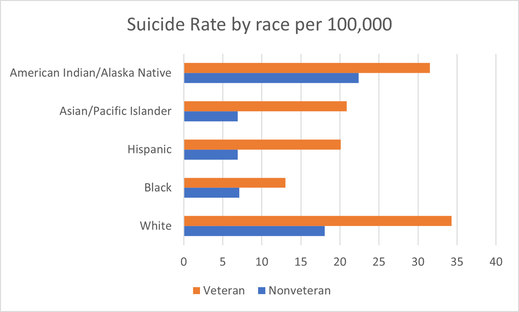
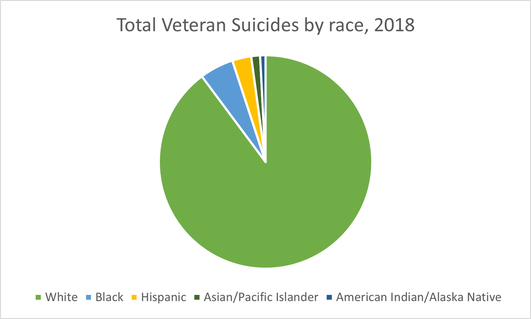
Appendix E- Location
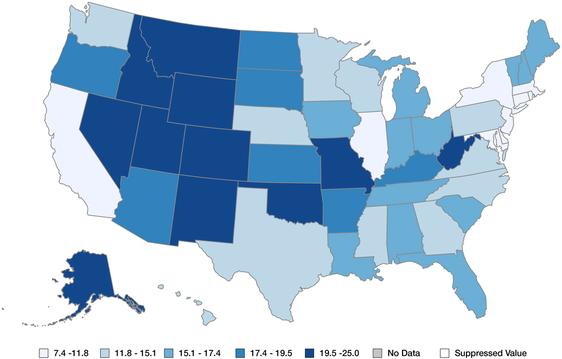
Works Cited:
|
|
